The Challenge of Building a Dermatology Lecture
Dermatology lectures look deceptively simple from the outside — show a few clinical photos, talk through a differential, finish with treatment. In practice, the prep tax is brutal. A melanoma grand rounds covering epidemiology, staging, and adjuvant therapy is a 35-slide deck that wants three separate visual languages: clinical photographs, dermoscopy and confocal images for the diagnosis sections, and survival curves and tumor-mutation pathway diagrams for the systemic-therapy sections. A Mohs surgery teaching talk needs surgical anatomy and intraoperative frozen-section images. A dermpath conference needs side-by-side H&E with immunostains.
You spend the night before licensing a representative ALM image, redrawing the AJCC 8th-edition staging table for the eighteenth time, and copy-pasting hazard ratios from the latest NEJM update on neoadjuvant nivolumab. By the time the deck looks like something a section chief will let you present, the literature has shifted again.
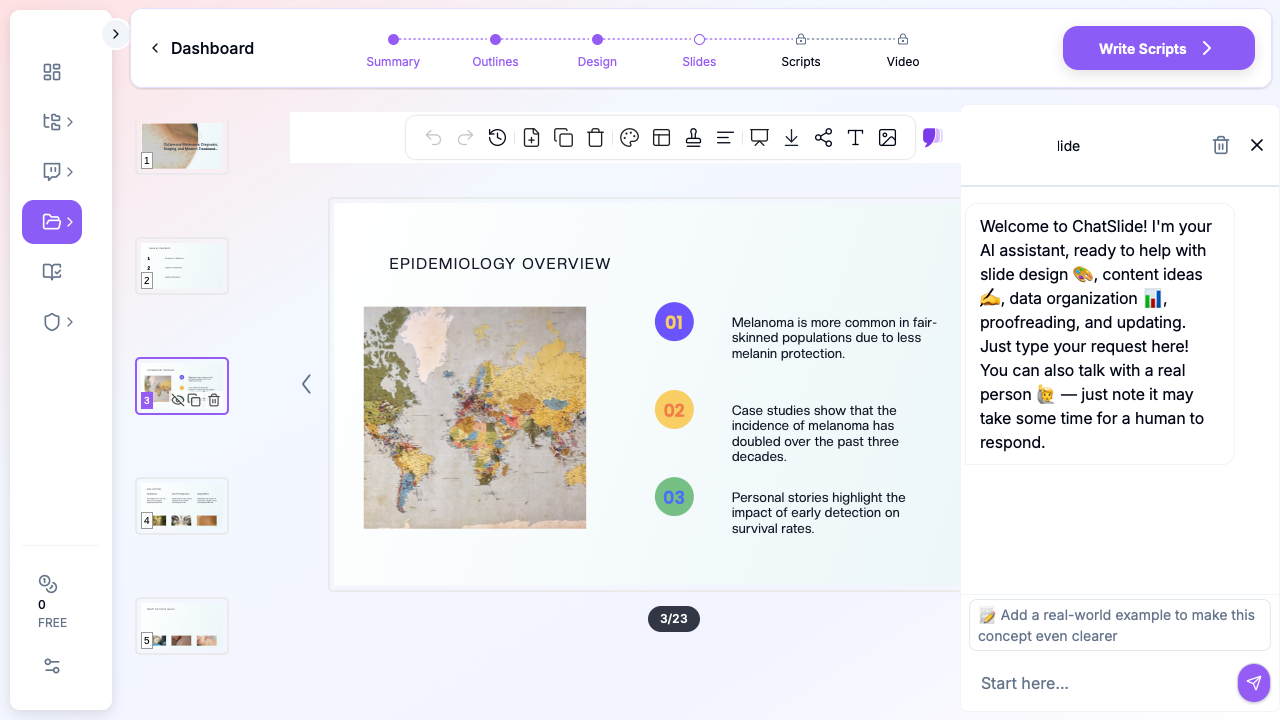
ChatSlide collapses that workflow. You hand it a topic — "Cutaneous melanoma: diagnosis, staging, and modern treatment" or "Dermoscopy of pigmented lesions for primary care" — and it returns a structured 30–40 slide deck with a clean clinical narrative, anatomy and pathology visuals, treatment-pathway diagrams, and per-slide speaker notes you can defend in front of a faculty audience.
What a Strong Dermatology Talk Actually Needs
Dermatology presentations are not just slide decks — they are visual diagnoses on a wall. A few non-negotiable elements separate a deck that survives a faculty room from one that gets quietly redirected:
A specific clinical entity, not a textbook chapter. "Skin cancer" is a chapter. "Acral lentiginous melanoma in skin of color: dermoscopic features and biopsy pitfalls" is a lecture. The sharper the entity, the cleaner the outline.
Clinical photographs that read in three seconds. A dermatology audience absorbs a clinical photo, dermoscopic image, or histology slide faster than any text bullet. Slides need representative imagery, not three bullets describing the lesion you should have shown.
Dermoscopy and visual-pattern slides. For pigmented lesions, melanoma differentials, or inflammatory dermatoses, dermoscopy or pattern-analysis figures often anchor the talk. Walk through the seven-point checklist or the two-step algorithm with a real lesion, not just a list of features.
Pathway slides for newer agents. Anti-PD-1, anti-LAG-3 (relatlimab), BRAF/MEK combinations, neoadjuvant immunotherapy in stage III, IL-17 / IL-23 / JAK inhibitors for inflammatory disease — your audience already knows the textbook receptor pathway. They want the new mechanism in one clean diagram with a callout where the drug acts.
Trial summaries that respect the audience. By the time you give a melanoma talk, every senior in the room has heard CheckMate, KEYNOTE, COLUMBUS, and SWOG acronyms many times. Show endpoints (RFS, OS, distant metastasis-free survival), durability curves, the toxicity signal that actually changes prescribing, and any biomarker subgroup that matters. Skip the CONSORT diagram.
A real case spine for grand rounds. Pre-biopsy clinical photo and dermoscopy → biopsy histology → staging workup → treatment course → follow-up. Three or four slides. The room engages the moment a real lesion appears.
A "what we do at our institution" slide. This is what separates a memorable dermatology talk from a guideline read-aloud. Whether it's a sentinel-lymph-node-biopsy threshold for thin melanoma, a dermoscopy referral algorithm, or a Mohs vs wide-local-excision decision tree — the audience wants a working algorithm, not a literature dump.
Step-by-Step: Building Your Dermatology Talk with ChatSlide
1. Pick a sharp scenario
In ChatSlide, choose Education > Lecture for a dermatology residency didactic, Conference > Keynote for an AAD or international congress talk, Education > Coursework for a med-school or PA-school dermatology lecture, or Education > Certification for board-prep review. The scenario biases the outline generator toward the right structure — entity-driven for didactics, case-driven for grand rounds, pattern-driven for dermoscopy CE.
2. Give it a clinical-question topic
Skip the textbook framing. Topics that work:
- "Cutaneous Melanoma: Diagnosis, Staging, and Modern Adjuvant Therapy"
- "Dermoscopy of Pigmented Lesions: Two-Step Algorithm with Cases"
- "Mohs Micrographic Surgery: Indications, Tissue Mapping, and Reconstructive Considerations"
- "Atopic Dermatitis in 2026: From Topical Steroids to Biologics and JAK Inhibitors"
- "Cutaneous T-Cell Lymphoma: Mycosis Fungoides Workup and Stage-Driven Treatment"
- "Adverse Cutaneous Drug Reactions: SJS/TEN and DRESS — A Practical Approach"
A topic with a verb in it — staging, diagnosing, managing, reconstructing — almost always produces a better outline than a noun phrase.
3. Define your audience precisely
"Dermatology PGY-2 residents at a Tuesday-morning didactic" produces a different outline from "primary care physicians at a regional CME on skin cancer screening." ChatSlide tunes the depth, the assumed background, and the level of mechanism detail to the audience field. For an AAD plenary, write "AAD 2026 plenary, attending dermatologists and fellows"; for a med-student lecture, name the rotation week.
4. Let it generate the outline first
Generate the outline before slides. The default 6 sections × 3 subpoints structure usually maps to: epidemiology and risk factors → clinical presentation and diagnostic clues → biopsy and pathology → staging or workup → treatment evidence → follow-up and surveillance. Edit any section name that drifts off-question. The outline is the cheapest place to fix structure.
5. Generate slides, then add images
Slide generation produces text + layout. The next step — image initialization — is the one that matters for a dermatology audience. ChatSlide pulls licensed stock visuals matched to your topic so your deck lands with anatomic context, clinical photography, and lab-bench imagery instead of placeholder graphics. Skip this step and the slides feel like a bare lecture-note dump. (For board-quality clinical photos and dermoscopy of specific entities, plan to swap in figures from your institution's case file or a licensed atlas — see the "Editing for clinical accuracy" tip below.)
6. Edit for clinical accuracy and visual quality
ChatSlide writes the structure and the obvious clinical scaffolding; you supply the judgment and the high-resolution dermatology imagery. Replace generic stock photos on the diagnosis slides with clinical and dermoscopic images from your own teaching file or a licensed atlas (DermNet, ASD, AAD's VisualDx). Update AJCC staging cutoffs, treatment thresholds, and hazard ratios from the latest update. Add your institution's biopsy thresholds, sentinel-node criteria, or Mohs indications where relevant. Spend editing time on the science and the visuals — not on slide mechanics.
7. Add speaker scripts for residency lectures
For residency didactics or board-prep lectures, the Scripts tab generates a per-slide speaker note. This is especially useful for residents giving their first didactic — the script gives a coherent narration to read off and adapt, instead of staring at a sparse outline at 6 a.m. before clinic.
Direct Research Database Access
ChatSlide's Research tab connects to the databases physicians use daily:
- PubMed: Search by keyword, PMID, or DOI. Find the landmark trials, recent publications, and clinical guidelines relevant to your case. The AI reads abstracts and incorporates key findings into your slides with citations.
- Google Scholar: When your topic spans disciplines — say, the intersection of genetics and oncology — Scholar captures the broader academic literature that PubMed alone might miss.
- Clinical Trials (NCT): Presenting on a treatment where pivotal trials are ongoing? Search by NCT number or condition to pull trial design, endpoints, and status into your slides.
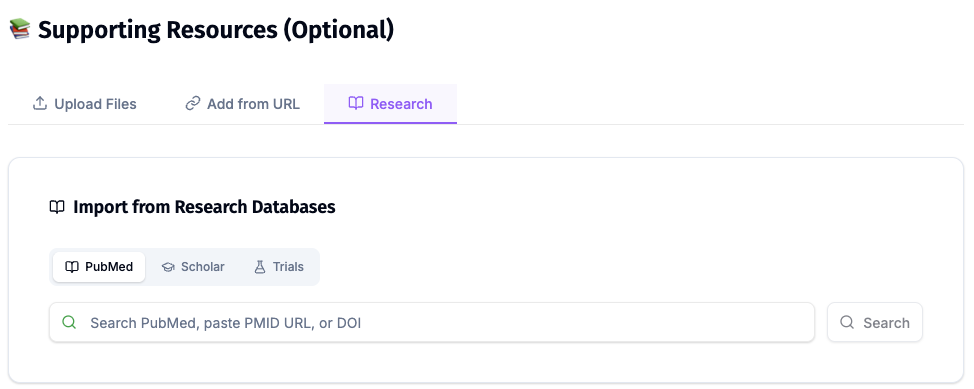
For a melanoma neoadjuvant talk, plug in the SWOG S1801 PMID, NADINA PMID, and the relevant CheckMate-067 long-term follow-up. ChatSlide reads the abstracts and produces speaker-ready slides with the trial design, endpoints, and key subgroup data already structured — saving the hour you would otherwise spend hand-translating PDFs into bullets.
Tips for Specific Dermatology Subspecialty Presentations
Pigmented lesions and melanoma. Lead with epidemiology and risk taxonomy (UV exposure, phenotype, genetic syndromes — CDKN2A, BAP1) before the clinical photos. Diagnosis slides should pair clinical photo, dermoscopy, and histology side-by-side; this is the visual triad faculty audiences expect. Treatment slides should follow stage I/II → stage III adjuvant → stage IV systemic, with a separate slide for neoadjuvant evidence — that is where most of the new data is.
Non-melanoma skin cancer (BCC, SCC). Build around an algorithm — biopsy → risk stratification (NCCN low/high) → treatment modality decision. A single high-yield slide on hedgehog inhibitors (vismodegib, sonidegib) for advanced BCC and immune checkpoint inhibitors (cemiplimab) for advanced SCC will land harder than a "Treatment" overview slide.
Mohs micrographic surgery. Open with indications, not technique. Audiences want to know when Mohs is the right modality before they want to see frozen-section interpretation. Reserve the technique deep-dive for a separate technique-focused talk; for general derm or referring providers, focus on indications, expected outcomes, and reconstructive options.
Dermoscopy CE and pattern analysis. Build the talk around lesions, not features. Each case slide should show a clinical photo, the dermoscopic image, the dermoscopic pattern call (asymmetric structures, atypical network, blue-white veil), and the histopathology after biopsy. A 30-minute dermoscopy talk with 6–8 well-chosen cases beats a 50-feature checklist every time.
Inflammatory dermatology (psoriasis, atopic dermatitis, hidradenitis). The last five years have been a biologics revolution. Build mechanism slides for IL-17 / IL-23 / IL-13 / JAK pathways and a sequencing slide for biologic and oral systemic options. End with patient-selection and access slides — most questions in the room will be about real-world prescribing.
Pediatric dermatology. Photo selection matters more here than anywhere. Conditions look different in skin of color and at different ages — your epidemiology and morphology slides need representative imagery across Fitzpatrick types I–VI. A separate slide on caregiver counseling and topical-steroid phobia tends to land well in pediatric CE rooms.
Dermatopathology conferences. Side-by-side H&E with immunohistochemistry is the central slide pattern. Build slide layouts that pair a low-power architecture image, a high-power cytology image, and the relevant IHC panel (Melan-A, SOX10, p53, p16, CD20, etc.) on a single slide. ChatSlide can scaffold the structure; you supply the histologic figures.
Drug reactions and dermatologic emergencies. SCORTEN, RegiSCAR DRESS criteria, and triggering-drug timelines are the high-yield content. A bedside-decision algorithm slide outperforms a long differential list for a busy hospital-medicine or emergency-medicine audience.
Cosmetic and laser dermatology CE. This audience wants device parameters, before/after photography, and complication management. ChatSlide can produce the didactic backbone (laser physics, chromophore targeting, Fitzpatrick-aware fluence selection) — you supply the procedural photographs and your settings.
Why This Workflow Beats Generic AI Slide Tools for Dermatology
Generic AI presentation tools fall down on dermatology in four predictable ways:
They ignore subspecialty taxonomy. A generic tool will produce "Treatment of skin cancer" — useless. ChatSlide's scenario presets push the model toward the structure the room expects: residency didactic vs CME plenary vs board review.
They drop visuals. A "create slides from topic" generic tool produces text-only decks or generic stock photos. ChatSlide's image initialization step is mandatory for dermatology — clinical photographs, dermoscopy, and histology all need visuals to land. (You will still swap in your own teaching-file imagery on the diagnosis slides; the goal is to never present text-only.)
They skip mechanism diagrams. Most generic tools cannot produce a coherent IL-23 / IL-17 / JAK / BRAF-MEK pathway slide. ChatSlide pulls licensed scientific imagery and can be edited with your own reference figures.
They produce slide-soup, not a clinical narrative. Dermatology talks have a story arc — entity, diagnosis, evidence, application. ChatSlide's outline-first flow forces narrative structure before slide generation.
Privacy and Patient-Data Hygiene
This is non-negotiable for dermatology decks, where clinical photographs are the central visual asset. Do not paste de-identified-but-still-recognizable patient photographs, faces, or identifying tattoos/landmarks into any AI tool. Use composites, licensed atlas images, or photos with documented teaching-use consent. ChatSlide is happy to generate cases from a stub — "62-year-old with a 1.4 mm ulcerated melanoma on the right calf, BRAF V600E mutated" — without ever seeing PHI or identifiable imagery. Your IRB and your patients will both prefer it.
A note on patient data and HIPAA: ChatSlide's standard plans are not a HIPAA-covered service — keep PHI, identifiable patient photographs, MRNs, and chart screenshots out of slide content, prompts, and uploads. For hospital systems, dermatology group practices, and academic departments that need a Business Associate Agreement, our Enterprise plan offers HIPAA-compliant deployment options — contact us to discuss BAA terms, SSO, and private-cloud or on-prem hosting.
Get Started
Whether you are a first-year dermatology resident building your first didactic, a Mohs fellow preparing a regional CE talk, an AAD plenary speaker writing a national keynote, or a community dermatologist running a primary-care skin-cancer-screening update — the slide-mechanics tax does not need to be your problem.
Start with ChatSlide.ai, pick the Education > Lecture or Conference > Keynote scenario, type your clinical entity as the topic, and generate. The deck you get back will not be the final talk — but it will be a much better starting point than a blank PowerPoint at 9 p.m. the night before grand rounds.
Try it for your next dermatology presentation — residency didactic, AAD talk, Mohs CE, dermoscopy lecture, or dermpath conference — and put your editing time where it belongs: on the science and the imagery.