Quick Answer: A useful otolaryngology deck usually needs (1) a focused anatomy primer — middle ear ossicles, paranasal sinuses, larynx, neck triangles — relevant to the topic, (2) clinical assessment — otoscopy, tuning forks, nasal endoscopy, flexible laryngoscopy, audiogram interpretation, (3) differential diagnosis with imaging cues (HRCT temporal bone, CT sinuses, MRI for IAC and skull base), (4) a stepwise management pathway — medical first, then procedural escalation, (5) surgical technique when relevant — approach, key landmarks, complications, (6) outcomes and follow-up with audiometric or symptom-based metrics, and (7) patient or parent counseling. Target 22–30 slides for a residency didactic, 12–18 for a CME workshop, 6–10 for a patient handout. ChatSlide accepts your PDFs and produces this structure with otologic and head-and-neck imagery rather than generic medical stock photos.
The Otolaryngology Slide Problem
ENT spans more anatomical territory than almost any other surgical specialty — ear, balance system, paranasal sinuses, nasal airway, oral cavity, oropharynx, larynx, salivary glands, neck, thyroid, skull base — and a single residency week can swing from a congenital microtia consult on Monday to a Zenker diverticulum case on Wednesday and an OSA sleep-study review on Friday. Generic presentation tools assume a "hospital keynote" template and produce wide-angle stock images of stethoscopes and operating-room ceilings. None of that survives a head-and-neck audience.
Make the deck the old way and a single Saturday morning lecture on "Congenital aural atresia and microtia reconstruction" eats the weekend: hunting for a clean middle-ear ossicular chain diagram, finding a labeled Jahrsdoerfer score reference, drawing the BAHA vs autologous reconstruction decision tree by hand in PowerPoint, and copying audiogram conventions out of a textbook. The deck is half-built and the talk is Monday morning.
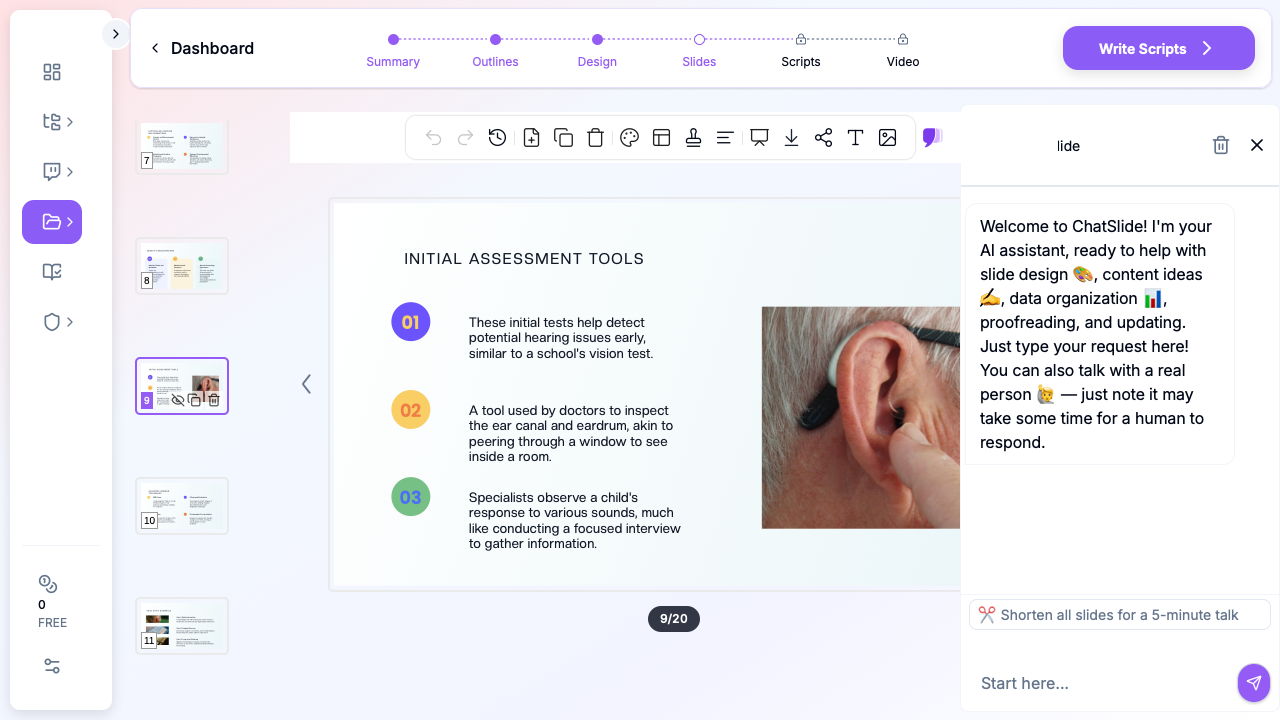
ChatSlide collapses the assembly. Drop a topic — "Congenital ear malformations: workup and reconstructive options" or "Endoscopic sinus surgery for chronic rhinosinusitis with nasal polyposis" — and you get a structured deck with relevant anatomy, side-by-side surgical approach comparisons, audiometric reference patterns, and counseling slides. You stay in charge of the clinical decisions and your own de-identified endoscopy stills; the tool stops eating your weekend.
What a Strong ENT Deck Actually Needs
Otolaryngology audiences span PGY-1 residents on their first ear-mastoid rotation, head-and-neck oncology fellows preparing tumor-board cases, audiology and speech-language pathology trainees, ENT attendings doing CME for their Foundation/ABOto board recertification, primary-care referrers needing a tonsillectomy-indication refresher, and parents trying to understand why their two-year-old needs tympanostomy tubes. Each room needs different things, but every strong otolaryngology deck shares the same backbone:
Anatomy that matches the diagnosis. A cholesteatoma talk needs the middle ear cleft, pars flaccida and pars tensa, ossicular chain with the long process of the incus marked, and the relationship to the lateral semicircular canal and facial nerve — not a generic "ear" cartoon. A FESS lecture needs the osteomeatal complex, ethmoidal bulla, agger nasi, frontal recess, and orbital relationships. The anatomy slide is the slide the rest of the lecture rests on; skip it and the audience loses the why.
Audiogram or endoscopy reference patterns when the topic demands them. Conductive vs sensorineural vs mixed loss is the foundational pattern recognition for any otology talk. A normal vs cobblestoned vs ulcerated laryngoscopy view is the foundational pattern for laryngology. The slide should show the pattern, not describe it.
Imaging slides with the planes the surgeon actually orders. Temporal bone HRCT in axial and coronal planes, with the Pöschl and Stenvers reformats called out when superior semicircular canal dehiscence is on the differential. Sinus CT in coronal with the Lund–Mackay scoring grid overlay. MRI IAC for vestibular schwannoma workup. Don't paste an "abdominal CT" stock image into an ENT deck.
A staged management pathway, not a binary "medical vs surgical" slide. Otolaryngologic disease is usually a ladder — watchful waiting → topical or oral medical therapy → in-office procedure → outpatient OR procedure → revision or salvage surgery. Show the ladder. A chronic otitis media with effusion deck shows: observation for 3 months → hearing test → tympanostomy tubes if persistent and hearing-affected → adenoidectomy on repeat tubes → consideration of T-tubes for recurrent disease. The ladder beats two prose bullets.
Surgical technique slides with landmarks, not just steps. A tympanoplasty slide should call out the chorda tympani, the facial recess, the round window niche, the long process of the incus. A thyroidectomy slide should show the recurrent laryngeal nerve, the inferior thyroid artery, the parathyroids. Landmarks are how residents learn; steps without landmarks are how residents fail their oral boards.
Audiometric or symptom-based outcome metrics. "Patient did well" is not a residency-quality outcomes slide. Pure-tone average pre/post tympanoplasty, air-bone gap closure, SNOT-22 reduction after FESS, VHI-10 change after vocal cord medialization, Glasgow Benefit Inventory for ear surgery — the outcome slide names the instrument and the clinically meaningful change.
Counseling slides written at a 6th-grade reading level when the audience is patients or parents. "Failure to treat may result in conductive hearing loss" is too vague. "Your child's ear fluid has not cleared after three months. We recommend placing small tubes that drain the fluid and let the ear pop normally. The tubes fall out on their own in 6 to 18 months. Hearing usually improves within a few days." Specific lands; abstract bounces off.
Image-rich without being a stock-photo gallery. Otoscopy stills, tympanic membrane diagrams, endoscopy stills, axial/coronal CT cuts, audiogram traces, surgical landmark photos, BAHA/cochlear implant device photos. Skip the generic stethoscope-and-clipboard shot — head-and-neck audiences tune it out.
Step-by-Step: Building Your ENT Lecture with ChatSlide
1. Pick the right scenario
In ChatSlide, choose Education > Lecture for residency didactics, ABOto / Foundation board prep, audiology or speech-language pathology coursework, or in-department staff training. The outline generator biases toward the primer → anatomy → assessment → management ladder → surgical technique → outcomes → cases structure that residency didactics expect.
For a single-condition parent-facing or patient-facing handout (tonsillectomy expectations, tympanostomy tube care, post-FESS instructions), switch to Customer Education > Patient Training. The structure tightens to one condition, one anatomy diagram, what we're doing, what to expect, when to call.
For an AAO-HNSF or COSM conference keynote, use Conference > Keynote — it adds the title slide, disclosures slide, learning objectives, and high-density evidence summary slides that conference audiences expect. For a fellowship tumor-board case (papillary thyroid cancer with central neck recurrence, parotid pleomorphic adenoma with deep-lobe extension, oropharyngeal SCC HPV+), Conference > Case generates the case-history → imaging → pathology → management discussion → outcomes shape.
2. Write the topic the way you'd describe it to your resident
Generic strings produce generic decks. Compare:
- Bad: "Ear lecture"
- Better: "Cholesteatoma diagnosis and surgical management"
- Best: "Acquired cholesteatoma — pathogenesis, otoscopic findings, HRCT cues, canal-wall-up vs canal-wall-down mastoidectomy decision-making, and 6-month/2-year follow-up imaging — 50-min PGY-3 didactic"
The third version gives the AI enough to build a 26-slide deck weighted correctly for mid-level residents — heavier on surgical decision-making, lighter on basic anatomy.
3. Define the audience precisely
"Residents" and "patients" produce different decks. Be explicit:
- "PGY-1 otolaryngology residents on their first pediatric ENT rotation"
- "PGY-3 residents preparing for their otology mock oral exam"
- "Head and neck oncology fellows in a first-year multidisciplinary tumor board"
- "Audiology AuD students learning cochlear implant candidacy assessment"
- "Pediatricians and family-medicine referrers learning OME and tympanostomy tube indications"
- "Parents of a 14-month-old scheduled for bilateral myringotomy with tube placement"
- "Adult patients with newly diagnosed chronic rhinosinusitis considering FESS"
A PGY-1 deck spends three minutes on tympanic membrane anatomy; a parent-facing tube deck spends 20 seconds and pivots to "what we do in the OR and what you watch for at home."
4. Generate the outline first
Outline generation is fast. Read the section structure before committing to slides. Common otolaryngology edits:
- Add an "imaging" section if it didn't surface — a head-and-neck deck without imaging is half a deck
- Combine redundant primer sections (one ossicular chain anatomy slide is enough for a tympanoplasty talk)
- Move the "complications" slide before "post-op care," not after — residents need to know what to watch for as they're operating
- For a procedure-focused deck (FESS, thyroidectomy, parotidectomy, microtia repair), add a "consent and counseling" section before the technique slides
- For board prep, add a "high-yield pearls" closing — Foundation/ABOto questions cluster around predictable mechanisms (CHARGE association, branchial arch derivatives, ototoxic medications, recurrent laryngeal nerve anatomy)
5. Generate slides with images
This is the step where generic AI tools fall down hardest on ENT topics. They produce text slides with stock-photo doctors holding clipboards. ChatSlide's image step pulls in otologic anatomy diagrams, otoscopy reference views, sinus and temporal-bone CT reformats, audiogram traces, and head-and-neck surgical landmark visuals — the kind of imagery otolaryngologic audiences expect.
For modality-specific imaging (your own tympanic membrane photos, intra-op endoscopy stills, a patient's HRCT temporal bone showing scutum erosion, an audiogram with a classic Carhart notch), swap in your own de-identified images. The deck structure stays intact — drag your screenshots into the existing image slots. De-identify at the source; ChatSlide does not see your raw DICOMs or patient identifiers.
6. Refine for the room
A 50-minute residency didactic for eight PGY-3s reads differently than an 8-minute pre-op counseling talk for a parent in clinic. Tighten the deck for the room:
- PGY-1 didactic: 24–30 slides, image-heavy, one anatomy refresher slide
- PGY-3 mock oral prep: 18–22 slides, decision-tree heavy, complications-front-and-center
- Fellowship tumor board case: 12–18 slides, history → imaging → path → multidisciplinary recommendations
- ABOto / Foundation board review: 15–20 high-density slides, exam-style MCQs every 10 minutes
- AAO-HNSF / COSM conference keynote: 25–35 slides, evidence-heavy, disclosures and learning objectives up front
- Parent education (in-office, pre-op tubes / adenoids): 6–10 slides, large text, what we do, what to expect, when to call
- Audiology / SLP coursework: 30–40 slides, audiogram-heavy, normative-data references
- Primary-care referrer CME: 14–20 slides, indication-focused, "when to refer" callouts
7. Export to PPTX or present from the browser
Exported PPTX preserves layout, bullets, and image positions — useful when grand rounds AV requires a local file. The browser preview also works well for in-clinic parent counseling where you want to swap a slide live based on which question the parent is asking.
Specific Use Cases This Replaces
Congenital aural atresia and microtia reconstruction. Embryology of the first and second branchial arches, classification systems (Marx, Weerda), Jahrsdoerfer score for surgical candidacy, BAHA vs autologous rib graft (Brent / Nagata stages) vs Medpor framework, audiometric outcomes, parental counseling timeline. Strong residency or fellowship deck — also adaptable to a parent-counseling shortened version.
Otitis media with effusion and tympanostomy tube placement. AAO-HNSF clinical practice guideline summary, three-month watchful waiting rationale, hearing test thresholds, surgical technique with myringotomy knife/needle and tube selection, tube-care counseling (water precautions, expected extrusion timeline). Front-desk-printable patient handout version possible.
Cholesteatoma — acquired and congenital. Pars flaccida vs pars tensa retraction pockets, HRCT cues (scutum erosion, ossicular erosion, lateral semicircular canal fistula), canal-wall-up vs canal-wall-down mastoidectomy, recurrence surveillance imaging (DWI-MRI), 6-month and 2-year follow-up protocols.
Endoscopic sinus surgery for chronic rhinosinusitis. Anatomy of the osteomeatal complex, EPOS guideline summary, role of medical therapy first, Lund–Mackay CT scoring, surgical steps (uncinectomy, maxillary antrostomy, anterior/posterior ethmoidectomy, frontal recess), complications (CSF leak, orbital injury), SNOT-22 outcome tracking.
Pediatric tonsillectomy and adenoidectomy. AAO-HNSF clinical practice guideline indications (recurrent throat infection criteria, obstructive sleep apnea), surgical techniques (cold-steel, electrocautery, coblation, intracapsular), post-op bleed risk by technique, pain control protocols, fluid-intake counseling for families. Strong companion patient-handout deck.
Vestibular schwannoma (acoustic neuroma) workup. Asymmetric SNHL screening criteria, MRI IAC with and without contrast, observation vs stereotactic radiation vs middle fossa vs translabyrinthine vs retrosigmoid approach, hearing preservation rates, facial nerve outcomes. Multidisciplinary skull-base tumor-board case format.
Cochlear implant candidacy assessment. Audiometric criteria, FDA labeling vs CMS coverage, AzBio sentence scoring, surgical technique (cochleostomy vs round window approach), device selection conversation, activation timeline and rehabilitation. Strong audiology lecture and parent-counseling formats.
Vocal cord paralysis and medialization laryngoplasty. Recurrent laryngeal nerve anatomy and common iatrogenic causes (thyroidectomy, mediastinal surgery), stroboscopy findings, VHI-10 baseline, injection laryngoplasty (carboxymethylcellulose, calcium hydroxylapatite, fat) vs framework medialization (Isshiki Type I), outcomes.
Thyroidectomy for differentiated thyroid cancer. ATA risk stratification, hemi vs total thyroidectomy decision, central neck dissection indications, recurrent laryngeal nerve and parathyroid identification, post-op calcium monitoring and TSH suppression targets, RAI ablation referral criteria. Strong head-and-neck oncology fellow deck.
Obstructive sleep apnea — surgical pathway. Drug-induced sleep endoscopy findings, anatomy-targeted surgery (UPPP, maxillomandibular advancement, hypoglossal nerve stimulation eligibility), STAR trial summary for HNS, AHI outcome targets. Cross-disciplinary deck for sleep medicine referrers.
BAHA / bone-anchored hearing systems. Candidacy (single-sided deafness, conductive losses unsuitable for tympanoplasty, microtia/atresia), audiometric workup, surgical placement under local vs GA, post-op care, expected audiometric benefit. Parent and adult versions both useful.
Direct Research Database Access
ChatSlide's Research tab connects to the databases physicians use daily:
- PubMed: Search by keyword, PMID, or DOI. Find the landmark trials, recent publications, and clinical guidelines relevant to your case. The AI reads abstracts and incorporates key findings into your slides with citations.
- Google Scholar: When your topic spans disciplines — say, the intersection of genetics and oncology — Scholar captures the broader academic literature that PubMed alone might miss.
- Clinical Trials (NCT): Presenting on a treatment where pivotal trials are ongoing? Search by NCT number or condition to pull trial design, endpoints, and status into your slides.
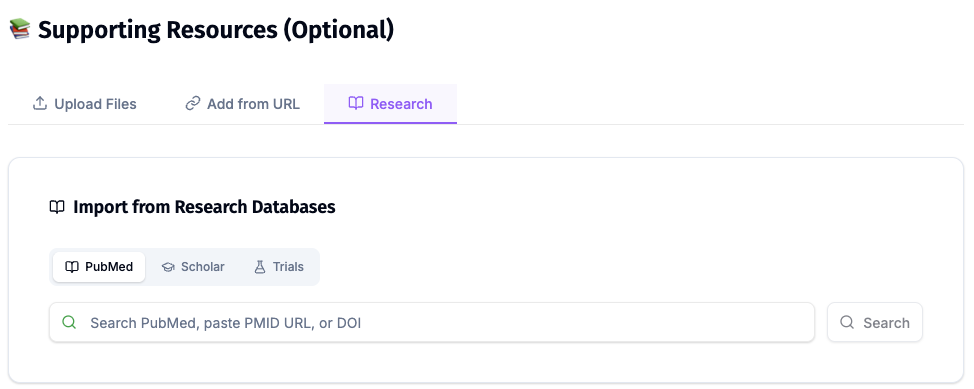
For otolaryngology specifically, the Research tab is most useful for pulling in the AAO-HNSF clinical practice guidelines (tonsillectomy, OME, sudden SNHL, Bell's palsy), the EPOS chronic rhinosinusitis position paper, the ATA thyroid nodule and thyroid cancer management guidelines, the STAR trial (Stimulation Therapy for Apnea Reduction) for hypoglossal nerve stimulation, and the major cochlear implant outcome series.
Tips Specific to Otolaryngology Lectures
Lead with the patient's question, not the anatomy. Parents walk in asking "why does my child keep getting ear infections?" — open the deck with that question, then let the anatomy slide answer it (eustachian tube angle in young children, lymphoid hyperplasia, daycare exposure). Residents respond to the same framing; oral-board scenarios land harder when they answer a clinical question.
Show the audiogram, don't describe it. A single annotated audiogram showing a Carhart notch teaches otosclerosis-related pseudo-SNHL in a way that a paragraph cannot. Same for a noise-notch at 4 kHz, a high-frequency presbycusis slope, and a typical cookie-bite congenital pattern. ChatSlide accommodates audiogram image inserts cleanly.
Mark the staged management ladder visibly. A horizontal ladder showing watchful waiting → medical therapy → in-office procedure → outpatient OR → revision surgery beats four prose bullets. Patients and residents both reference it.
Put complications on their own slide. A FESS deck should have a single high-contrast complications slide — CSF leak, orbital hematoma, lamina papyracea breach, anterior ethmoidal artery injury, skull-base entry — with a brief management note for each. Residents memorize this slide before the oral exam.
Use the right imaging plane. Temporal bone disease lives on the HRCT axial and coronal; vestibular schwannoma lives on the MRI IAC; sinus disease lives on the coronal CT; thyroid nodules live on ultrasound with TI-RADS scoring; head-and-neck cancer lives on the contrast-enhanced neck CT. Match the plane to the diagnosis.
Cite AAO-HNSF, EPOS, and ATA guidelines where applicable. Society-endorsed pathways carry weight with referring PCPs, with peer reviewers, and with payers reviewing prior authorizations. A footer reference to the AAO-HNSF tonsillectomy CPG is worth two extra bullets of evidence prose.
Avoid the stethoscope-and-clipboard slide. Generic medical stock photos signal you didn't put time into the talk. Otoscopy stills, temporal-bone diagrams, paranasal sinus drawings, laryngoscopy stills, audiogram traces, surgical landmark photos — that's the visual vocabulary head-and-neck audiences expect.
Build a 6-slide patient-handout version of every procedure. Once your residency deck on tympanostomy tubes is built, clone it into a parent-facing 6-slide PDF. ChatSlide makes the duplication and audience swap a two-minute step. Your front desk hands the PDF out at check-out; parental adherence to water precautions and follow-up tympanometry goes up.
Why Generic AI Presentation Tools Underperform Here
Most AI deck generators were built for sales pitches and marketing decks. They optimize for visual flair and ignore the structural conventions of clinical didactics — and especially the conventions of head-and-neck medicine. For an otolaryngology audience, generic tools produce:
- Anatomy slides that show "an ear" or "a sinus" without labeling the specific structure the diagnosis lives in (scutum, lateral semicircular canal, frontal recess, agger nasi, ossicular chain)
- Management slides that collapse a four-step ladder into a single "medical vs surgical" binary
- Surgical technique slides that skip the consent and complications steps and jump straight to the cutting
- Stock-photo "doctor reviewing chart" slides that have no place in a parent-counseling tympanostomy-tube talk
- No imaging slides at all, or generic abdominal-CT clip art pasted into a temporal-bone deck
ChatSlide's clinical scenarios — Education > Lecture, Customer Education > Patient Training, Conference > Keynote, Conference > Case — bias the output toward the conventions head-and-neck audiences actually expect. You're still the clinical author; the tool just stops fighting your format.
Get Started
Building your next otolaryngology lecture, tumor-board case, or parent-counseling handout on ChatSlide takes about as long as a clinic follow-up visit. Drop a topic, refine the outline, generate the slides with otologic and head-and-neck imagery, swap in your own de-identified otoscopy stills or CT cuts, and you have a residency-ready, board-prep-ready, or parent-ready deck before the next half-day clinic block.
Try it free at chatslide.ai — most ENT residency programs and head-and-neck attendings go from blank screen to first draft in under fifteen minutes.
Related guides:
- AI Medical Presentation Maker for Healthcare Professionals
- Pediatric Medicine Presentation AI Guide
- Patient Education Presentation AI Guide
- Medical Grand Rounds Presentation AI Guide
- Dermatology Presentation AI Guide
A note on patient data and HIPAA. ChatSlide's standard plans are not a HIPAA-covered service — keep PHI out of slide content, prompts, and uploads. De-identify your audiograms, CT cuts, endoscopy stills, and case data before you import. For hospital systems, multi-site ENT groups, and academic otolaryngology programs that need a Business Associate Agreement, our Enterprise plan offers HIPAA-compliant deployment options — contact us to discuss BAA terms, SSO, and private-cloud or on-prem hosting.