Quick Answer: A strong movement disorders deck usually needs (1) a focused functional anatomy slide — basal ganglia circuits, direct/indirect/hyperdirect pathways, dopaminergic pathways — sized to the topic, (2) phenomenology with video-style frame stills — rest vs action tremor, hypokinetic vs hyperkinetic bullets, MDS-UPDRS reference, (3) diagnostic workup — DaTscan, MRI patterns, genetic panels (GBA, LRRK2, Parkin), supportive features per MDS criteria, (4) a staged management ladder — non-motor optimization, levodopa initiation, dopamine agonists, MAO-B and COMT inhibitors, advanced therapies (LCIG, apomorphine, DBS, focused ultrasound, transcranial pulse stimulation), (5) device and neuromodulation slides with target nuclei (STN, GPi, VIM) and stimulation parameters, (6) outcome measures — UPDRS III, PDQ-39, ON/OFF diaries, dyskinesia scores, and (7) patient/care-partner counseling. Target 22–30 slides for a fellowship lecture, 12–18 for an MDS satellite symposium, 6–10 for a clinic handout. ChatSlide reads your PDFs (trial papers, guideline documents, your DBS programming notes) and produces this structure with neuroanatomy-relevant imagery instead of generic brain-and-stethoscope stock.
The Movement Disorders Slide Problem
A movement disorders clinic week can swing from a newly diagnosed Parkinson's disease patient on Monday to a Tourette syndrome teen on Tuesday, a refractory cervical dystonia botulinum-toxin clinic on Wednesday, an STN-DBS programming session on Thursday, and an MDS-affiliated didactic on Friday about transcranial pulse stimulation. The lectures, case conferences, and tumor-board-style multidisciplinary reviews that come out of that clinic land in the same generic AI presentation tools that ship "Modern Business Pitch" and "Sleek Education" templates — and the output reflects it.
Build a movement disorders deck the old way and one Saturday on "Advances in non-invasive neuromodulation for Parkinson's disease" eats the weekend: re-drawing the basal ganglia circuit diagram in PowerPoint shapes, hunting for a clean DaTscan reference image with anonymized eccentricity, copying MDS-UPDRS subscores out of a PDF appendix, and trying to find a stimulation-parameter side-by-side for STN vs GPi vs VIM that doesn't look like a 2009 textbook scan. The deck is half-built and the symposium is Monday morning.
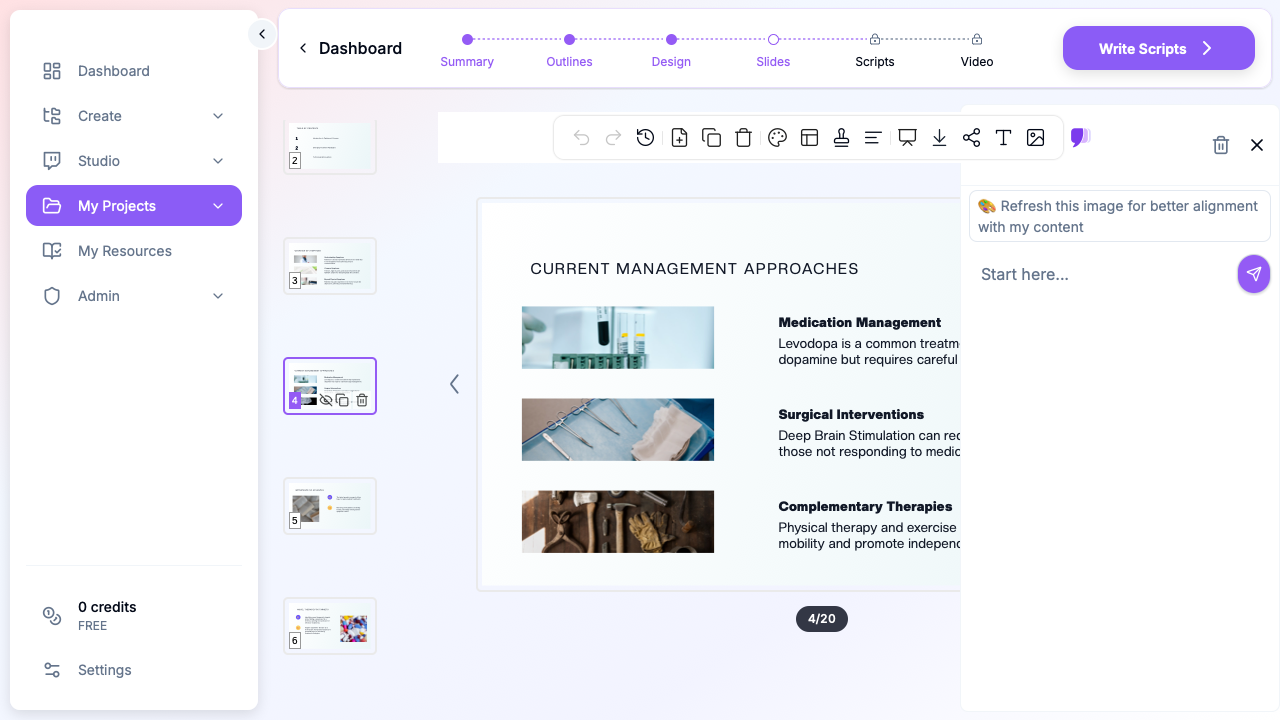
ChatSlide collapses that assembly. Drop in a topic — "Transcranial pulse stimulation in idiopathic Parkinson disease" or "Programming the subthalamic nucleus DBS lead: a fellowship primer" — and you get a structured deck with circuit-relevant anatomy, ON/OFF response timelines, neuromodulation device comparisons, and outcome-instrument tables. You stay in charge of the clinical judgment, your de-identified patient videos, and your institution's stimulation protocols; the tool stops eating the weekend.
What a Strong Movement Disorders Deck Actually Needs
Movement disorders audiences span PGY-2 neurology residents on their first movement clinic rotation, MDS fellows preparing case conferences, neurosurgeons reviewing DBS candidacy, neuropsychologists scoring pre-op cognitive panels, allied-health PT/OT/SLP teams running LSVT BIG and LOUD programs, MDS attendings doing CME for ABPN MOC, primary-care referrers needing a "when to refer for tremor" refresher, and care partners trying to understand what motor fluctuations actually mean. Each room needs different things, but every strong movement disorders deck shares the same backbone:
Anatomy that matches the diagnosis. A Parkinson disease talk needs the substantia nigra pars compacta with dopaminergic projections to the striatum, the direct/indirect pathway loop through GPi/SNr and thalamus, and the hyperdirect cortico-subthalamic pathway — not a generic "brain" cartoon. A cervical dystonia talk needs the splenius capitis, levator scapulae, scalene complex, and SCM, with the corticostriatal sensorimotor integration model on the etiology slide. A DBS lecture needs the STN with the motor, associative, and limbic territories color-coded against the lead trajectory. Skip the circuit slide and the audience loses the why behind every subsequent therapy choice.
Phenomenology with video-still references. Rest tremor at 4–6 Hz vs postural/action tremor at 8–12 Hz looks different from a still image but reads differently in bullets too. A good slide pairs the phenomenology bullet with a stylized still frame and the relevant MDS-UPDRS or TETRAS reference subscore. Hyperkinetic vs hypokinetic, focal vs segmental vs generalized dystonia, simple vs complex tics — pattern recognition is the curriculum.
Diagnostic slides that show what the supportive feature actually looks like. DaTscan with asymmetric putaminal uptake reduction (the "comma" becoming a "period"). MRI brain with the "hummingbird" sign in PSP or the "hot-cross-bun" in MSA-C. Genetic-panel result formats showing GBA, LRRK2, Parkin, PINK1, SNCA. MDS clinical diagnostic criteria for PD as a flowchart, not a paragraph.
A staged management ladder, not a binary "medical vs surgical" slide. Movement-disorders therapeutics is a ladder — non-motor symptom optimization (constipation, REM sleep behavior disorder, depression) → levodopa initiation with side-effect counseling → dopamine agonists with impulse-control disorder caution → MAO-B and COMT add-on for wearing-off → continuous dopaminergic delivery (LCIG, apomorphine pump, foslevodopa-foscarbidopa) → advanced therapies (DBS, MR-guided focused ultrasound, transcranial pulse stimulation in selected patients). Show the ladder. The "what's next when levodopa stops working" slide is more useful than another mechanism-of-action figure.
Neuromodulation slides with targets, parameters, and complication profiles. STN-DBS for the motor-fluctuating PD patient; GPi-DBS when dyskinesia or cognitive concerns dominate; VIM-DBS or focused ultrasound thalamotomy for tremor-predominant disease; thalamic stimulation for essential tremor; pallidal or thalamic targets for dystonia; transcranial pulse stimulation as a non-invasive option under active investigation. Each slide names the target nucleus, the typical starting amplitude/frequency/pulse width, and the side-effect profile (paresthesias, dysarthria, mood, cognitive). Residents and fellows learn from parameter tables, not from prose.
Outcome instruments named explicitly. "Patient improved" is not a movement-disorders outcomes slide. MDS-UPDRS Part III on/off scores, PDQ-39 quality-of-life subscores, UDysRS for dyskinesia, TETRAS for essential tremor, Toronto Western Spasmodic Torticollis Rating Scale for cervical dystonia, Yale Global Tic Severity Scale for Tourette. The outcome slide names the instrument and the clinically meaningful change.
Counseling slides written at a 6th-grade reading level when the audience is patients or care partners. "Motor fluctuations may occur" is too vague. "Your levodopa starts working about 30 minutes after you take it and lasts about 4 hours. Over time, that window gets shorter. When the window is less than 3 hours, we add medicines that stretch each dose. If those stop working, we talk about a pump or DBS." Specific lands; abstract bounces off.
Image-rich without being a stock-photo gallery. Basal ganglia circuit diagrams, DaTscan stills, MRI patterns, DBS lead trajectories, programming-screen reference images, MDS-UPDRS instrument formats, device photos (DBS implantable pulse generators, focused-ultrasound rigs, transcranial pulse stimulation headsets), patient video stills when permissioned. Skip the generic "brain made of glowing lines" stock — movement-disorders audiences tune it out.
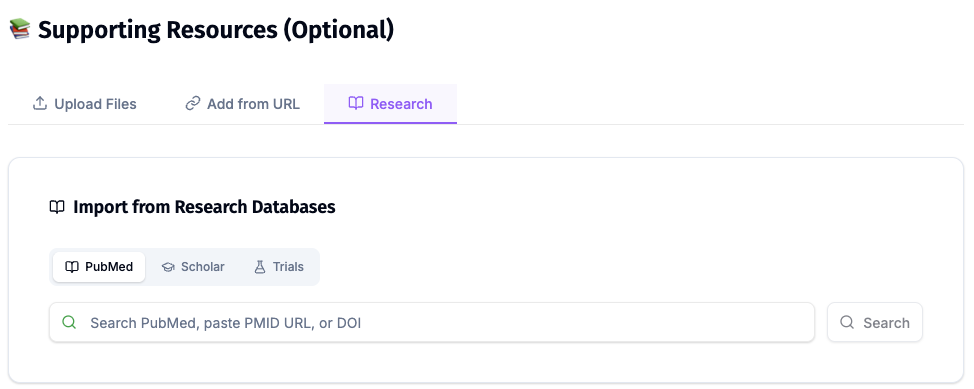
Direct Research Database Access
ChatSlide's Research tab connects to the databases physicians use daily:
- PubMed: Search by keyword, PMID, or DOI. Find the landmark trials, recent publications, and clinical guidelines relevant to your case. The AI reads abstracts and incorporates key findings into your slides with citations.
- Google Scholar: When your topic spans disciplines — say, the intersection of neuromodulation engineering and clinical movement disorders — Scholar captures the broader literature that PubMed alone might miss.
- Clinical Trials (NCT): Presenting on focused ultrasound for tremor or transcranial pulse stimulation for PD? Search by NCT number or condition to pull trial design, endpoints, and status into your slides.
For a movement-disorders fellowship lecture on, for example, "Subthalamic vs pallidal DBS for advanced Parkinson disease," the workflow looks like this: pull the NSTAPS, COMPARE, and CSP-468 papers from PubMed by PMID; pull the most recent guideline papers (MDS task force statements) by DOI; pull active comparative-efficacy NCTs that involve directional leads or sensing-enabled IPGs. Every claim on the slide carries a citation, and the references slide is auto-built from what the AI actually used — no more chasing down citations the night before the talk.
Step-by-Step: Building Your Movement Disorders Lecture with ChatSlide
1. Pick the right scenario
Choose Education > Lecture for fellowship didactics, ABPN MOC modules, allied-health teaching for PT/OT/SLP, or in-department case conferences. The outline generator biases toward the anatomy → phenomenology → workup → management ladder → device parameters → outcomes → cases structure that fellowships expect.
For an MDS satellite symposium or a single-paper conference deck, switch to Conference > Keynote. The structure tightens to background → motivating clinical problem → methods → results → discussion → take-home points, with a heavier emphasis on the headline outcome figure and the speaker-notes script.
For a one-condition patient or care-partner handout (post-DBS programming visit instructions, levodopa wearing-off worksheet, fall-prevention sheet), switch to Customer Education > Patient Training. The structure tightens to one diagnosis, one anatomy diagram, what we're doing, what to expect, when to call.
2. Drop in your source materials
Upload your PDFs — landmark trial papers (CAPS-PD, EARLYSTIM, PD-MED), the MDS clinical diagnostic criteria document, your institution's DBS programming SOP, recent transcranial pulse stimulation publications, your own case summary. ChatSlide reads the PDFs and uses them as the factual backbone of the deck. Add a typed prompt for the angle: "Fellowship audience. Emphasize when to refer for advanced therapy. Cover STN vs GPi vs VIM and where focused ultrasound and transcranial pulse stimulation fit in 2026." Specific intent shapes the outline.
3. Refine the outline before generating slides
After ChatSlide drafts the outline, scan it for the slides you actually need. Add a "Phenomenology in 90 seconds" early slide. Add a "When to refer for DBS" slide before the device section. Move "Complications of stimulation" before the "Programming for dyskinesia" slide so the fellow has the safety frame first. Outline edits cost seconds; slide edits cost minutes.
4. Generate the deck, then review against your clinical experience
ChatSlide writes the slides with anatomy diagrams, MRI/DaTscan reference imagery, device and neuromodulation comparisons, and outcome-instrument tables. Review every clinical claim — the model will draft useful starting language but the attending owns the recommendation. Swap stock anatomy for your own anonymized DaTscan, MRI, or DBS-lead screenshots when you have them; the slide template holds the layout.
5. Add a video for the talk-style version
For an MDS satellite symposium or a recorded CME module, use the Video tab to add narration and a presenter avatar. Movement-disorders audiences travel; on-demand video lets fellows in different time zones see the same lecture.
Tips for Movement Disorders Presentations
Name the diagnostic criteria you're using. MDS Clinical Diagnostic Criteria for PD (2015), MDS Research Criteria for Prodromal PD, Movement Disorder Society Task Force criteria for atypical parkinsonisms — say which set on the slide. Movement disorders audiences are criteria-literate and the implicit framing matters.
Show the response, not just the drug. A "levodopa" mechanism slide is fine; a "levodopa response with morning akinesia, peak-dose dyskinesia, and end-of-dose wearing-off" timeline is the slide that teaches fluctuating disease.
Distinguish tremor types early. Rest vs action vs intention vs orthostatic tremor live in different therapeutic worlds. A two-by-two grid of phenomenology vs anatomical localization is a single slide that prevents 20 minutes of confusion later.
Pair every device with a parameter table. STN-DBS: typical 2.5–3.5 V (or 2–3 mA), 130 Hz, 60 μs. GPi-DBS: 2.5–3.5 V, 130 Hz, 90 μs. VIM: 1.5–3 V, 130–180 Hz, 60 μs. Numbers belong on the slide; the fellow will photograph it.
Show the non-motor slide. Constipation, hyposmia, REM sleep behavior disorder, depression, orthostatic hypotension, cognitive change. Half of patient burden lives here and most lectures skip it. A movement-disorders deck that includes a non-motor slide reads as written by someone who runs clinic.
Counsel about impulse-control disorders when dopamine agonists appear. Pathological gambling, hypersexuality, compulsive shopping, punding. The slide that names them is the slide that saves a marriage. Always pair the agonist slide with the ICD-screening prompt.
Build a "when to refer" slide for primary-care referrers. Tremor without other parkinsonian features, possible essential tremor failing first-line medication, rapidly progressive parkinsonism, atypical features (early falls, early autonomic failure, gaze palsy), DBS candidacy. Specific referral criteria turn a CME lecture into a referral-pattern shift.
For DBS programming sessions, use ON/OFF testing slides. A pre/post-stim TUG time, MDS-UPDRS Part III ON/OFF subscores, dyskinesia diary excerpts — the programming room is data-dense and the slide should match.
Note on patient data: ChatSlide's standard plans are not a HIPAA-covered service — keep PHI, identifiable DBS programming records, and protected video out of slide content and uploads. For hospital systems, neuroscience institutes, and academic medical centers that need a Business Associate Agreement, our Enterprise plan offers HIPAA-compliant deployment options — contact us to discuss BAA terms, SSO, and on-prem / private-cloud hosting for fellowship-program materials and de-identified patient registries.
Get Started
Movement disorders neurology rewards slide craft. Fellows learn from circuit diagrams and parameter tables. Care partners hold onto specific counseling language. Conference audiences remember the headline outcome figure. ChatSlide gives you a backbone deck in minutes so the Saturday morning before a Monday MDS-affiliated symposium goes back to your kids — not to redrawing the basal ganglia loop in PowerPoint shapes.
Try ChatSlide free and turn your next Parkinson's, tremor, dystonia, or DBS lecture into a finished, properly cited deck this afternoon.