Quick Answer: A useful podiatry deck usually needs (1) a clinical anatomy primer — plantar fascia, sesamoids, posterior tibial tendon, lower-extremity vascular and neurologic supply, (2) etiology and biomechanics — pronation, equinus, Windlass mechanism, first-ray insufficiency, (3) examination findings — palpation, gait, single-leg heel rise, neurovascular and dermatologic checks, (4) a conservative pathway — orthotics, night splints, stretching, NSAIDs, immobilization, (5) procedural options — injections, chemical matrixectomy, casting, fixation, (6) patient education — what the patient does at home for 6–12 weeks, and (7) outcomes and follow-up. Target 18–28 slides for a residency didactic, 6–10 for a single-page patient handout deck. ChatSlide accepts your PDFs and produces this structure with foot-and-ankle imagery rather than generic medical stock photos.
The Podiatry Slide Problem
Foot-and-ankle medicine sits in an awkward gap. Generic medical-presentation tools assume you want a hospital-keynote feel — wide-angle stock photos of doctors in long white coats, a stethoscope as the visual motif. None of that fits a community podiatry practice or a residency program where the actual visuals you need are gait patterns, X-ray plates, casting technique, dermatologic findings on the foot, and step-by-step patient instructions.
Make the deck the old way and a single Sesamoiditis patient-education talk eats a Saturday: hunting for a clean sesamoid anatomy diagram, redrawing the Windlass mechanism, screenshotting a posterior night splint into a slide, and copying conservative-treatment timelines from your residency notes into bullet points. The lecture is half-built by Sunday afternoon.
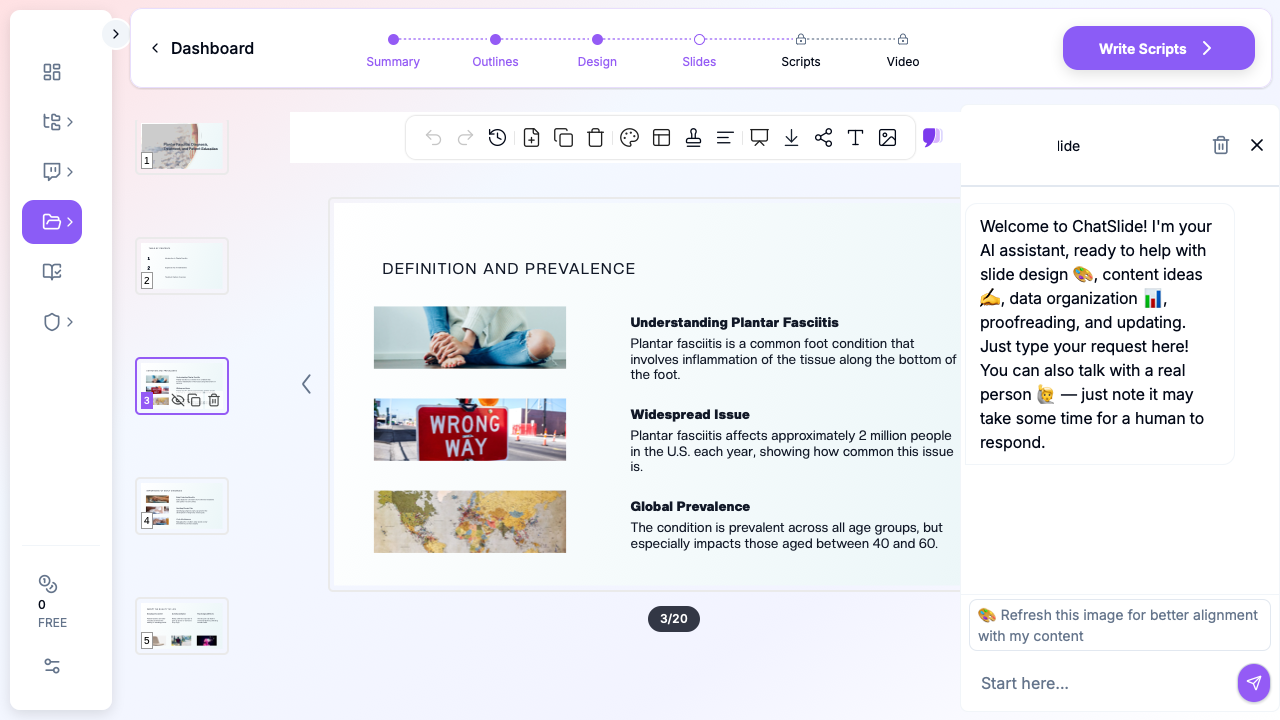
ChatSlide collapses the assembly. Drop a topic — "Plantar fasciitis: diagnosis and conservative treatment" or "Step-by-step chemical matrixectomy with phenol" — and you get a structured deck with anatomic visuals, side-by-side comparisons, and patient-ready instruction slides. You stay in charge of the clinical decisions and the de-identified imaging; the tool stops eating your weekend.
What a Strong Podiatry Deck Actually Needs
Podiatry audiences span a wide range: DPM residents in their PGY-1 didactics, board-prep candidates for the ABFAS or ABPM, community-practice podiatrists building patient handouts, sports medicine clinicians referring out to foot-and-ankle specialists, and patients who got handed a diagnosis they've never heard of. A strong podiatric deck has to hit a specific set of bars:
Anatomy that matches the diagnosis. A plantar fasciitis talk needs the plantar fascia origin at the medial calcaneal tubercle, not a stock image of "a foot." A sesamoiditis talk needs the tibial and fibular sesamoids under the first metatarsal head, with the flexor hallucis brevis and the cruciate ligament of the sesamoids visible. Anatomic precision is the floor, not a stretch goal.
Biomechanics framed as a cause, not a curiosity. The Windlass mechanism explains why first-step pain happens at the medial calcaneal tubercle. Equinus drives pronation, which drives plantar fascia overload. First-ray insufficiency overloads the second metatarsal head. The biomechanics slide isn't optional — it's the slide that earns the rest of your treatment plan.
Conservative pathway with realistic timelines. Most foot pathology improves with 6–12 weeks of structured conservative care. A residency-quality deck shows the timeline explicitly: weeks 0–2 (NSAIDs, ice, activity modification, taping), weeks 2–6 (orthotics, plantar stretching, night splint), weeks 6–12 (PT, ESWT if available, reassessment). Patients who see the timeline up front complete the protocol.
Procedure cards with clear pre/intra/post steps. A chemical matrixectomy slide should show: anesthesia (digital block, lidocaine without epi), tourniquet placement, nail avulsion, application of phenol vs sodium hydroxide, neutralization, dressing, post-op care. Same structure for posterior night splint application — application technique, wear schedule, expected first-week discomfort, when to call.
Patient-education slides written at a 6th-grade reading level. "Reduce activity that triggers symptoms" is too vague. "For the next two weeks: no running, no hiking, no jumping; walking and biking are fine; ice the heel for 15 minutes after any standing." Specific instructions land; abstractions don't.
Image-rich without being a stock-photo gallery. Foot diagrams, X-ray plates (de-identified), gait line views, orthotic device photos, casting and splint reference photos. Skip the stethoscope-and-clipboard cliché — podiatric audiences ignore it.
Coding and DME documentation when relevant. Residency and community-practice decks benefit from a short coding slide — L3000-series orthotic codes, E0181 vs L4396 night splint codes, the 11750 nail-avulsion code with matrixectomy modifier. Skip for patient-facing decks; include for clinical staff training.
Step-by-Step: Building Your Podiatry Lecture with ChatSlide
1. Pick the right scenario
In ChatSlide, choose Education > Lecture for residency didactics, ABFAS/ABPM prep, podiatry school courseware, or staff training. The outline generator biases toward the primer → principles → application → cases → summary shape that residency didactics expect.
For a single-condition patient handout, switch to Customer Education > Patient Training. The structure tightens to one diagnosis, one anatomy slide, one cause slide, a conservative plan, what to expect at follow-up, and red flags — the layout patients actually read.
For an academic conference talk (say, "Surgical correction of cavus foot deformity"), use Conference > Keynote. For a quality-improvement project on diabetic-foot infection rates, Research > Results generates the IRB-ready structure.
2. Write the topic the way you'd describe it to your resident
Generic strings produce generic decks. Compare:
- Bad: "Foot pain lecture"
- Better: "Plantar fasciitis diagnosis and treatment"
- Best: "Plantar fasciitis: diagnosis, biomechanics, conservative pathway, and ESWT — 45-min PGY-1 didactic with patient-counseling pearls"
The third version gives the AI enough to build a 22-slide deck weighted correctly for first-year residents — heavier on examination and biomechanics, lighter on advanced surgical options.
3. Define the audience precisely
"Residents" and "patients" produce different decks. Be explicit:
- "PGY-1 podiatry residents on their first lower-extremity rotation"
- "Third-year DPM students preparing for the APMLE Part II"
- "Community podiatrists pursuing ABPM recertification CME"
- "Adult patients newly diagnosed with plantar fasciitis at their first office visit"
- "Diabetic-foot clinic patients learning daily inspection and offloading"
A PGY-1 deck spends three minutes on the Windlass mechanism; a patient-facing deck spends 30 seconds and pivots to "what you do at home."
4. Generate the outline first
Outline generation is fast. Read the section structure before committing to slides. Common podiatric edits:
- Add a "biomechanics" section if it didn't surface — most generic AI tools skip it and the deck suffers
- Combine redundant primer sections (one plantar fascia anatomy slide is enough)
- Move the conservative-pathway timeline next to the patient-education slide, not three sections away
- For a procedure-focused deck (matrixectomy, posterior splint application, total contact casting), add a "consent and risks" section before the technique slides
- For ABFAS prep, add a "high-yield pearls" closing — boards questions cluster around predictable mechanisms
5. Generate slides with images
This is the step where generic AI tools fall down hardest. They produce text slides with stock-photo doctors holding clipboards. ChatSlide's image step pulls in foot anatomy diagrams, X-ray-style plates, orthotic device imagery, and gait-pattern visuals — the kind of imagery podiatric audiences expect.
For modality-specific imaging (your own intra-op photos, X-rays of the patient, MRI of partial plantar fascia tear), swap in your own de-identified images. The deck structure stays intact — drag your screenshots into the existing image slots. ChatSlide does not see your raw DICOMs or patient identifiers; de-identify at the source.
6. Refine for the room
A 45-minute residency didactic for six PGY-1s reads differently than an 8-minute patient education talk in your exam room. Tighten the deck for the room:
- PGY-1 didactic: 22–28 slides, image-heavy, one biomechanics algorithm slide
- ABFAS / ABPM board prep: 15–20 high-density slides, exam-style multiple-choice slides every 10 minutes
- Patient education (in-office): 6–10 slides, large text, clear timeline, red-flag callouts
- DPM school courseware: 30–40 slides per topic, anatomy-heavy, references to the primary literature
- CME workshop: 20–25 slides, hands-on stations (casting, splinting, injection landmarks), less text per slide
- Diabetic foot clinic staff training: 12–18 slides, protocol-heavy, photo-driven
7. Export to PPTX or present from the browser
Exported PPTX preserves layout, bullets, and image positions — useful when the conference room AV requires a local file. The browser preview also works well for in-room patient education where you want to swap a slide live based on what the patient is asking.
Specific Use Cases This Replaces
Plantar fasciitis patient counseling. Anatomy, Windlass mechanism, first-step pain explanation, conservative pathway timeline, night splint instructions, "when to call us" red flags. The 6-slide version becomes a printable handout your front desk hands out at check-out.
Sesamoiditis vs sesamoid fracture. Tibial vs fibular sesamoid anatomy, palpation findings, X-ray views (axial sesamoid view), MRI when indicated, conservative protocol (offloading, dancer's pad, immobilization), surgical excision criteria.
Achilles tendinitis (insertional vs non-insertional). Anatomy of the Achilles paratenon, retrocalcaneal bursa, Haglund's deformity, conservative pathway with eccentric loading protocol, ESWT, PRP discussion, surgical options for refractory cases.
Chemical matrixectomy step-by-step. Patient selection (recurrent ingrown nail), anesthesia (digital block), tourniquet, nail avulsion, phenol vs sodium hydroxide vs surgical Winograd, neutralization, dressing, post-op timeline. Strong residency teaching deck — also a useful patient-education shortened version.
Posterior night splint application. Indication (plantar fasciitis, equinus contracture), sizing, application technique, expected first-week discomfort, wear schedule (overnight only, not during ambulation), troubleshooting (pressure points, sleep disruption). Train your medical assistants once; reuse the deck for every new patient.
Diabetic foot daily inspection. Inspection technique, mirror use, what counts as a wound, when to call (any new wound, any redness extending beyond the wound, fever, malaise), offloading basics, footwear recommendations. Fits the 8-minute exam-room window.
Below-knee fiberglass cast application. Stockinette and padding technique, fiberglass roll mechanics, molding the foot in neutral, drying time, cast care instructions for the patient, cast saw safety briefing for staff. Strong residency procedural deck.
Achilles tendinopathy ESWT counseling. What ESWT is, evidence base summary, treatment schedule (typically 3 weekly sessions), expected response timeline, what continues alongside (eccentric loading), what does not (steroid injections in tendon body).
Plantar plate injury vs Morton neuroma. Differential diagnosis flow, examination findings (Mulder's click, vertical stress test of MTP, paper-pull test), imaging selection, conservative pathway, surgical referral criteria.
Direct Research Database Access
ChatSlide's Research tab connects to the databases physicians use daily:
- PubMed: Search by keyword, PMID, or DOI. Find the landmark trials, recent publications, and clinical guidelines relevant to your case. The AI reads abstracts and incorporates key findings into your slides with citations.
- Google Scholar: When your topic spans disciplines — say, the intersection of genetics and oncology — Scholar captures the broader academic literature that PubMed alone might miss.
- Clinical Trials (NCT): Presenting on a treatment where pivotal trials are ongoing? Search by NCT number or condition to pull trial design, endpoints, and status into your slides.
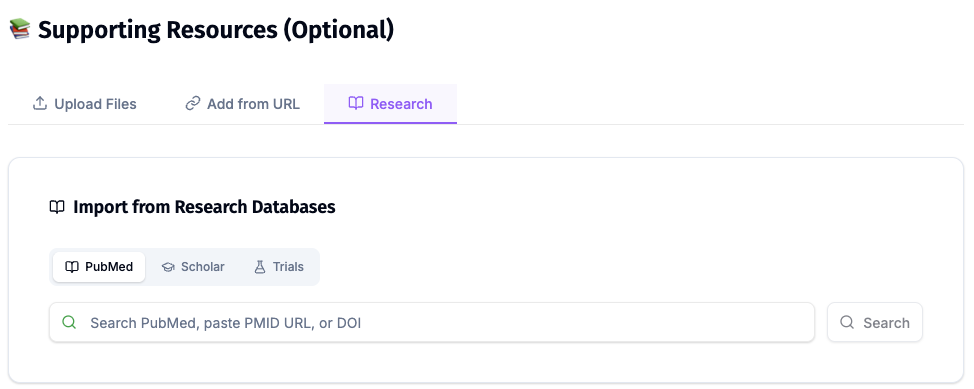
For podiatry specifically, the Research tab is most useful for pulling in the foundational plantar fasciitis treatment trials (DiGiovanni et al. on plantar fascia stretching), the IDSA diabetic foot infection guidelines, the ACFAS clinical consensus statements on conditions like hallux valgus and posterior tibial tendon dysfunction, and the major ESWT systematic reviews.
Tips Specific to Podiatry Lectures
Lead with the patient's question, not the anatomy. Patients walk in asking "why does my heel hurt every morning?" — open the deck with that question and let the anatomy slide answer it. Residents respond to the same framing; ABFAS pearls land harder when they answer a clinical question.
Show gait, don't describe gait. A 5-second gait video clip teaches pronation in a way that a paragraph cannot. If you have a de-identified gait clip, the deck should accommodate a video slide. ChatSlide handles MP4 inserts without re-encoding mangling.
Mark the conservative timeline visibly. Patients want to know "how long until I'm better." Residents need to memorize the trial timepoints. A horizontal timeline with weeks 0 / 2 / 6 / 12 marked beats four prose bullets.
Put red flags on their own slide. Cauda equina-style red flags for foot pathology — increasing redness, fever, new ulcer in a diabetic, sudden inability to bear weight on the Achilles — go on a single high-contrast slide. Patients and front-desk staff both reference it.
Cite ACFAS and APMA where applicable. Society-endorsed pathways carry weight with referring PCPs and with payers reviewing prior authorizations. A footer reference to the ACFAS consensus statement is worth two extra bullets of evidence prose.
Avoid the stethoscope-and-clipboard slide. Generic medical stock photos signal you didn't put time into the talk. Foot anatomy, X-ray imagery, orthotic device photos, casting reference shots, gait line drawings — that's the visual vocabulary podiatric audiences expect.
Build a 6-slide patient-handout version of every condition. Once your residency deck on Achilles tendinitis is built, clone it into a patient-facing 6-slide PDF. ChatSlide makes the duplication and audience swap a two-minute step. Your front desk hands the PDF out at check-out; patient adherence to conservative protocols goes up measurably.
Why Generic AI Presentation Tools Underperform Here
Most AI deck generators were built for sales pitches and marketing decks. They optimize for visual flair and ignore the structural conventions of clinical didactics — and especially the conventions of foot-and-ankle medicine. For a podiatric audience, generic tools produce:
- Anatomy slides that show "a foot" without labeling the specific structure the diagnosis lives in
- Conservative-pathway slides without timelines, so patients hear "do these stretches" without knowing for how long
- Procedure slides that skip the anesthesia step and jump to the cutting
- Stock-photo "doctor reviewing chart" slides that have no place in an in-office patient education talk
- No biomechanics section at all, which guts the why behind everything else
ChatSlide's clinical scenarios — Education > Lecture, Customer Education > Patient Training, Conference > Keynote — bias the output toward the conventions podiatric audiences actually expect. You're still the clinical author; the tool just stops fighting your format.
Get Started
Building your next podiatry lecture or patient handout on ChatSlide takes about as long as a follow-up visit. Drop a topic, refine the outline, generate the slides with foot-and-ankle imagery, swap in your own de-identified X-rays or intra-op photos, and you have a residency-ready or patient-ready deck before the next half-day clinic block.
Try it free at chatslide.ai — most DPMs and podiatric residency programs go from blank screen to first draft in under fifteen minutes.
Related guides:
- AI Medical Presentation Maker for Healthcare Professionals
- Patient Education Presentation AI Guide
- Patient Education Leaflet AI Handout Maker
- Medical Grand Rounds Presentation AI Guide
- Dental Lecture Presentation AI Guide
A note on patient data and HIPAA. ChatSlide's standard plans are not a HIPAA-covered service — keep PHI out of slide content, prompts, and uploads. De-identify your X-rays, intra-op photos, and case data before you import. For hospital systems, multi-site podiatry groups, and academic foot-and-ankle programs that need a Business Associate Agreement, our Enterprise plan offers HIPAA-compliant deployment options — contact us to discuss BAA terms, SSO, and private-cloud or on-prem hosting.