Quick Answer: A clinically-grounded psychotherapy training deck follows 5 sections: (1) Theoretical framework (CBT cognitive triangle, DBT diary card, IFS parts map, EMDR 8-phase, etc.), (2) Evidence base — RCTs, effect sizes, indicated populations, (3) Clinical skills demonstrated with scripted dialogue or role-play prompts, (4) Case conceptualization worked through end-to-end, (5) Ethics & cultural-responsiveness + post-test for CEU credit. Target 25–40 slides for a 3-hour CEU. ChatSlide takes your treatment manual or session-notes PDF and generates the framework diagrams + case conceptualization template.
The Challenge of Psychotherapy Presentations
Therapists, counselors, and clinical supervisors regularly find themselves preparing slide decks — for continuing education workshops, in-service trainings at agencies, case conceptualization rounds, supervision groups, and graduate-level coursework. Unlike a one-off lecture, these presentations have to do real clinical work: communicating evidence-based frameworks accurately, modeling ethical practice, and giving attendees something they can apply with the very next client they see.
The preparation challenge is unique to the field. A licensed clinical social worker putting together a six-hour CEU on trauma-informed care is balancing three things at once: covering enough theory to satisfy the licensing board, demonstrating clinical application through case vignettes, and pacing the material so a room full of fellow clinicians stays engaged across an entire afternoon. The slides have to support all three goals without becoming so text-heavy that they distract from the discussion the workshop is supposed to generate.
The other complication is that mental health content sits in a sensitive register. A presentation that uses real client stories crosses ethical lines. A presentation that uses only abstract diagnostic criteria feels disconnected from clinical reality. A presentation that includes graphic case material without trauma-informed framing can be retraumatizing for participants who themselves have lived experience. The slides have to walk a careful line between clinical specificity and ethical caution.
This is where most therapists end up spending hours fighting with PowerPoint when they would rather be developing the actual content. AI presentation tools, used thoughtfully, can take care of the structural and visual scaffolding so the clinician's energy goes into what only they can do: the case formulation, the ethical commentary, and the live discussion.
What Makes a Strong Psychotherapy Presentation
Presentations for mental health audiences have specific conventions that differ from corporate training, medical conferences, or general education talks. Getting these right signals clinical credibility.
Theoretical grounding before technique. Therapists are trained to think in terms of theoretical orientation — psychodynamic, cognitive-behavioral, humanistic, systemic, integrative. A presentation that jumps straight into techniques without grounding them in a coherent framework reads as superficial. Strong decks open with the relevant theory, then derive techniques from it, rather than the other way around.
Case conceptualization, not case stories. Rather than presenting identifiable client narratives, experienced presenters use composite or hypothetical cases to illustrate clinical decision-making. The format usually walks the audience through presenting concerns, hypothesized mechanisms, treatment planning, and intervention selection. This teaches clinical reasoning without compromising confidentiality.
Evidence base with appropriate humility. Clinicians want to know what the research says, but they also want a presenter who acknowledges the limits of that evidence. A slide claiming "CBT works for everyone" undermines credibility. A slide that says "CBT shows strong efficacy for major depression in adult outpatient samples, with effect sizes in the moderate range, though questions remain about long-term outcomes and cultural adaptation" earns trust.
Trauma-informed framing. Presentations on topics like trauma, suicide, eating disorders, or substance use should include a content warning at the start, pace difficult material gradually, and signal that participants can step out as needed. This is now standard practice in most clinical training contexts.
Cultural humility and applicability. Mental health interventions developed in WEIRD (Western, Educated, Industrialized, Rich, Democratic) populations don't always transfer cleanly to other contexts. Strong presentations acknowledge cultural considerations explicitly rather than treating them as an afterthought slide at the end.
Experiential learning prompts. The best CEU and training presentations include reflection questions, role-play prompts, or small-group discussion segments. Rather than three hours of lecture, the slides scaffold learning activities that let clinicians practice the new framework with each other.
Step-by-Step: Creating Psychotherapy Slides with ChatSlide
Here is the workflow for putting together a psychotherapy training presentation using ChatSlide, from initial topic to a ready-to-present deck.
Step 1: Define the Workshop Topic and Audience
Open ChatSlide and start a new project. The topic should be specific enough that the AI can build relevant content. Generic prompts like "therapy presentation" produce generic slides; specific prompts like "Cognitive Behavioral Therapy for Generalized Anxiety Disorder: A Three-Hour CEU Workshop" produce structured content with appropriate depth.
When defining the audience, be precise about clinical level. A presentation for first-year MFT graduate students differs significantly from one aimed at licensed clinicians with five years of post-licensure experience. ChatSlide adapts the depth and assumed background based on the audience description, so phrases like "licensed therapists with intermediate CBT familiarity" or "social work interns at a community mental health agency" yield better results than "therapists."
Step 2: Generate the Outline
ChatSlide's outline generator produces a section-by-section structure based on the topic. For a psychotherapy presentation, expect sections covering theoretical background, evidence base, core techniques, clinical application, and discussion prompts. Review the outline before generating slides — at this stage it is easier to add a section on cultural considerations or restructure the order than to do so after slides are generated.
For a CEU workshop, ensure the outline includes enough sections to fill the contact hour requirements without padding. A six-hour workshop typically needs eight to twelve substantive content sections plus opening and closing material.
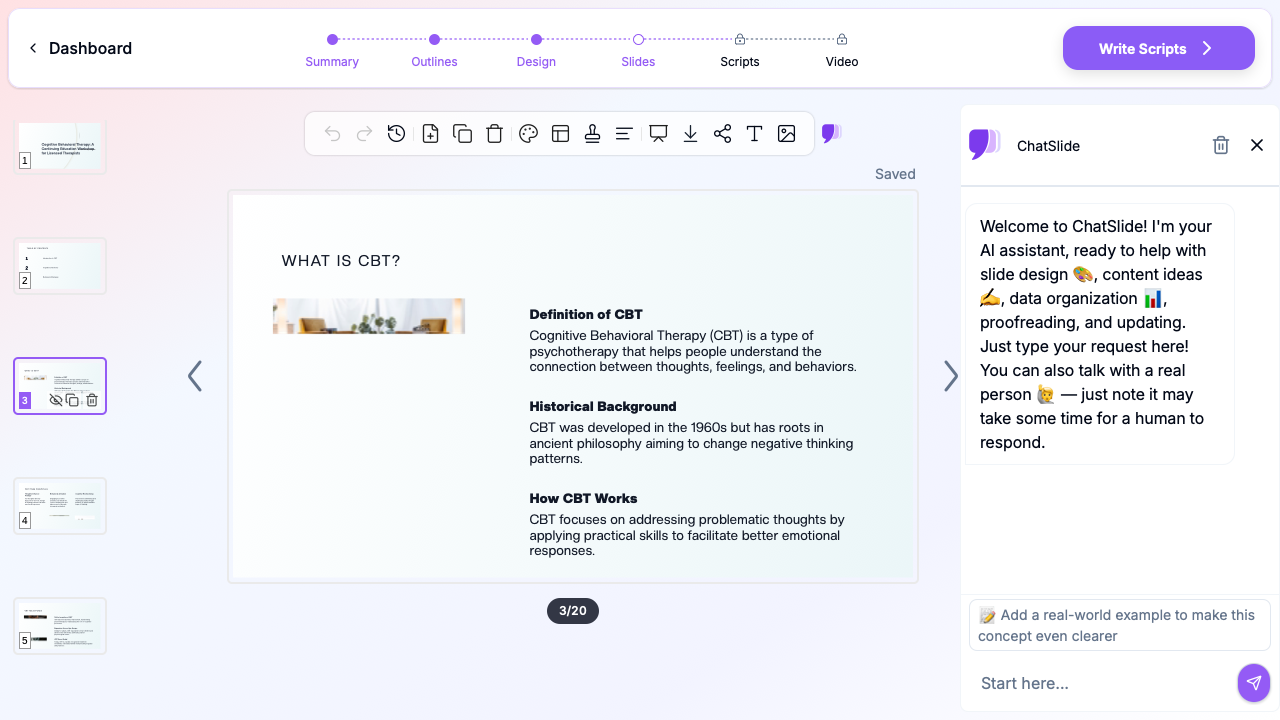
Step 3: Generate Slides with Visual Support
Once the outline is approved, ChatSlide generates slides with appropriate layouts, headers, and supporting visuals. Diagrams of cognitive models, treatment pathway flowcharts, and conceptual frameworks render automatically. The AI selects relevant stock imagery — a clinician at a desk, a therapy office, abstract representations of cognitive patterns — that fits clinical contexts without veering into stigmatizing or sensationalized territory.
Review the visual choices carefully. Stock photos that read as "happy person looking out the window" can undermine the seriousness of trauma content; stock photos that read as overly clinical can make a humanistic presentation feel cold. Swap images where the tone does not fit.
Step 4: Customize Theoretical Content
This is where the AI-generated framework meets your clinical expertise. Replace generic explanations of CBT, ACT, IFS, EMDR, or whatever modality is being presented with the specific language and emphasis your audience expects. If you are presenting to a CBT-trained audience, you can use technical terms like "cognitive restructuring" and "behavioral activation" without defining them; if you are presenting to a mixed audience, add definitions.
This is also where you add citations to seminal texts and current meta-analyses. ChatSlide gives you the structure; the citations and the specific evidence claims are yours to verify and add.
Step 5: Add Case Conceptualizations
Replace any AI-generated case examples with your own composite or hypothetical cases. The AI does not have access to real client information and will not produce identifiable narratives, but the cases it generates are generic. Your own composite cases — built from clinical experience but altered to be unrecognizable — will resonate more strongly with the audience and better illustrate the specific points you want to make.
A useful structure for case slides: presenting concerns, relevant history, hypothesized mechanism, treatment plan, and outcome or learning point. Keep cases consistent with the theoretical framework you have established earlier in the presentation.
Step 6: Add Discussion Prompts and Activities
The closing third of the presentation should include reflection questions, small-group discussion prompts, or role-play exercises. ChatSlide can generate initial discussion questions, but the most valuable prompts come from your own clinical experience. Questions like "How would you handle a client who refuses homework?" or "What countertransference might come up working with this presentation?" engage clinicians in a way that abstract review questions do not.
For longer workshops, build in experiential breaks every 60 to 90 minutes. Slides that say "Pair up and practice the cognitive restructuring sequence with a partner — 15 minutes" do more for skill acquisition than another lecture slide.
Step 7: Review for Ethical and Trauma-Informed Considerations
Before finalizing, do a deliberate pass for ethical considerations. Add content warnings to any slides covering trauma, suicide, abuse, or other heavy material. Ensure no client information could be identifiable. Check that examples reflect diverse populations rather than defaulting to a single demographic. Confirm that any clinical claims are appropriately hedged and supported by current evidence.
This pass takes ten minutes and is what separates a competent presentation from a clinically trustworthy one.
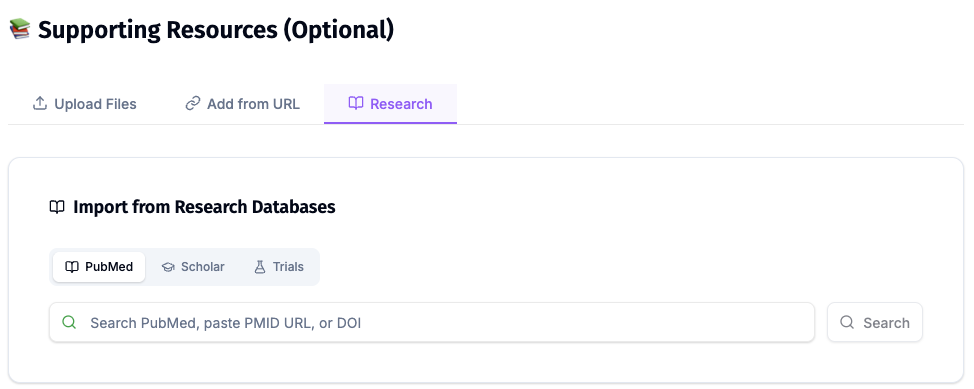
Direct Research Database Access
ChatSlide's Research tab connects to the databases physicians use daily:
- PubMed: Search by keyword, PMID, or DOI. Find the landmark trials, recent publications, and clinical guidelines relevant to your case. The AI reads abstracts and incorporates key findings into your slides with citations.
- Google Scholar: When your topic spans disciplines — say, the intersection of genetics and oncology — Scholar captures the broader academic literature that PubMed alone might miss.
- Clinical Trials (NCT): Presenting on a treatment where pivotal trials are ongoing? Search by NCT number or condition to pull trial design, endpoints, and status into your slides.
Tips for Different Psychotherapy Presentation Types
Different presentation contexts call for different emphases.
CEU workshops require board-approved learning objectives stated explicitly at the beginning, time blocked out for breaks per board requirements, and a closing slide summarizing how to claim CE credit. Many licensing boards now require a learning assessment, so build in three to five review questions at the end.
Clinical supervision groups are smaller and more intimate. Slides should be sparse — supervision is a discussion, not a lecture. Use the deck to scaffold case presentations, frameworks for parallel process or countertransference, and reflective prompts. Five to fifteen content slides is usually enough for a 90-minute group.
Graduate-level coursework lectures can carry more content because students are accountable for absorbing it. Include reading citations on each conceptual slide so students can follow up. Build in case applications throughout rather than only at the end.
Agency in-service trainings need to be highly applied. The audience is clinicians who will see clients next week, so prioritize techniques and decision rules over abstract theory. Include a one-page handout slide that summarizes the key takeaways for clinicians to keep at their desks.
Community psychoeducation talks are different again — the audience is non-clinicians, often family members or community members. Slides should use accessible language, avoid clinical jargon, and emphasize practical understanding over theoretical depth. Always include resources and how to access mental health support at the close.
Get Started with Psychotherapy Slides
Mental health professionals have less time than the demands of practice would suggest. Documentation, billing, supervision, continuing education, and direct service all compete for the same hours. Creating a high-quality presentation should not consume an entire weekend.
ChatSlide handles the structural and visual work of building a psychotherapy presentation in minutes — generating the outline, drafting the slides, sourcing visuals, and producing a coherent deck — so the clinician's preparation time goes into the case formulation, the ethical framing, and the live workshop facilitation. The result is presentations that look polished, communicate clinical content accurately, and leave room for the human connection that distinguishes mental health work in the first place.
Open the ChatSlide app to start your next CEU workshop, supervision deck, or training presentation. Whether you are preparing a three-hour CBT workshop, a graduate seminar on family systems theory, or a clinical supervision group, the platform handles the slide-building so you can focus on the clinical thinking.
A note on patient data and HIPAA. ChatSlide's standard plans are not a HIPAA-covered service — keep PHI out of slide content, prompts, and uploads. For hospital systems, group practices, and clinics that need a Business Associate Agreement, our Enterprise plan offers HIPAA-compliant deployment options — contact us to discuss BAA terms, SSO, and private-cloud or on-prem hosting.