Quick Answer: A useful spine surgery deck usually needs (1) clinical anatomy — bony landmarks, neural elements, disc and endplate anatomy, posterior tension band, (2) pathology and natural history — degeneration cascade, Modic changes, spondylolisthesis grading (Meyerding, Wiltse), deformity Lenke/SRS-Schwab classification, (3) examination and imaging workup — neurologic exam, provocative tests, plain films with flex/ex, MRI signal characteristics, dynamic and standing imaging, (4) non-operative pathway — PT, ESI, RFA, BVNA, when conservative care has been "adequate," (5) surgical options compared head-to-head — ALIF vs posterior fusion, decompression-only vs decompression-plus-fusion, MIS vs open, (6) outcomes data — fusion rates, PROs (ODI, VAS, SF-36), reoperation rates with confidence intervals, and (7) complications and avoidance. Target 25–35 slides for a NASS/AAOS instructional course, 18–22 for a fellowship didactic, 10–12 for a tumor-board or M&M case. ChatSlide accepts your PDFs and outlines this structure with spine-specific imagery and side-by-side technique comparisons.
The Spine Slide Problem
Spine surgery presentations sit in an unusually demanding visual category. A fusion-technique comparison deck needs paired lateral lumbar images, intra-op photos of disc-space preparation, cage and screw renderings, and outcome plots — none of which a generic AI deck tool produces. Drop "ALIF vs posterior fusion for L4-5 isthmic spondylolisthesis" into a marketing-AI deck builder and you get a slide of a smiling patient holding their back, three sentences of LLM-generated background, and a "Future Outlook" slide. Useless for a NASS instructional course, useless for a fellowship didactic, and embarrassingly useless next to the technique videos and PROs tables the spine community expects.
Make the deck the old way and a single ALIF-vs-posterior comparison talk eats an entire weekend: hunting for clean L4-5 sagittal MRIs, redrawing the Wiltse classification, screenshotting cage and pedicle-screw renderings, and copying ODI/VAS outcomes out of three Spine and Journal of Neurosurgery: Spine PDFs into a comparison table. Sunday night arrives, you have 30 slides of bullets, and the comparison table you actually need still doesn't exist.
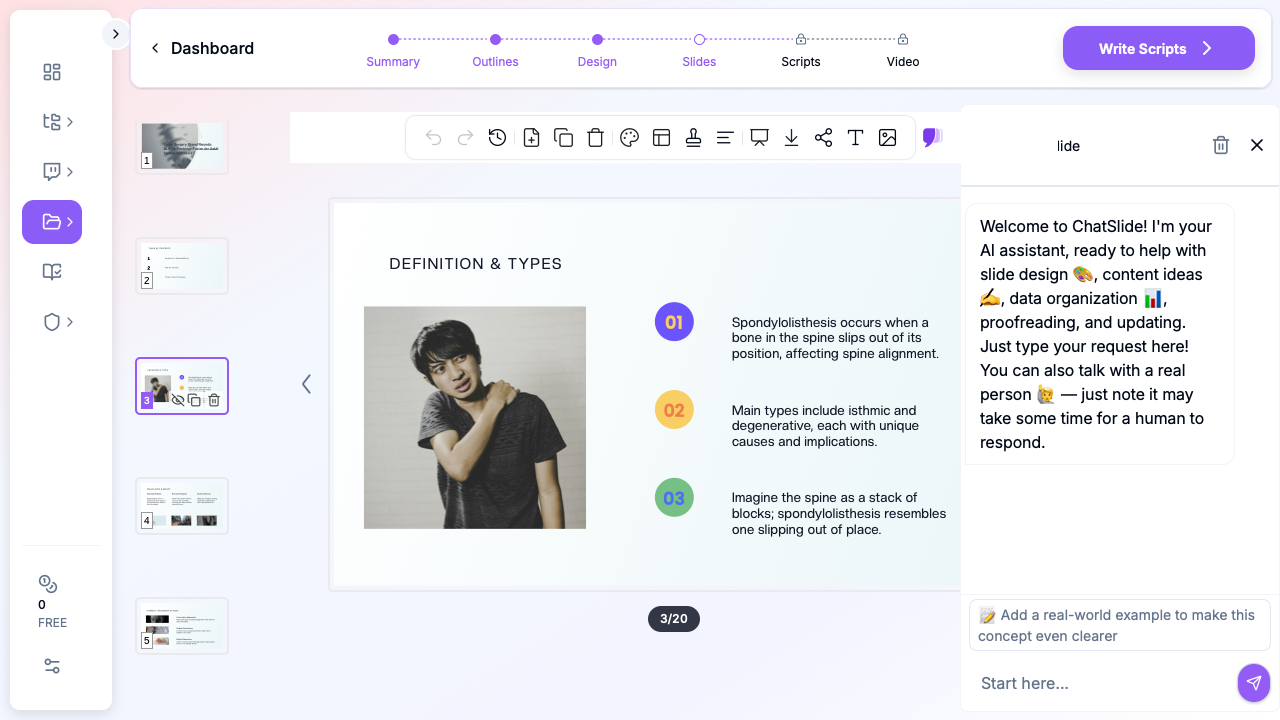
ChatSlide collapses the assembly. Drop a topic — "ALIF with posterior fixation vs posterior osteotomy and fusion for L5-S1 high-grade dysplastic spondylolisthesis" or "Modic Type 1 changes: basivertebral nerve ablation indications and 2-year outcomes" — and you get a structured deck with anatomic visuals, technique-comparison tables, and outcomes slides ready to drop in your own intra-op imagery. You stay in charge of the surgical judgment and the de-identified imaging; the tool stops eating your weekend.
What a Strong Spine Surgery Deck Actually Needs
Spine audiences span a wider technical range than almost any other surgical subspecialty. An orthopedic spine fellow needs different framing than a neurosurgery spine fellow, a NASS instructional-course audience splits between MIS-leaning surgeons and open traditionalists, a tumor board mixes oncology and spine, and an M&M conference expects a precise root-cause framing. A strong spine deck has to hit a specific set of bars:
Anatomy slides that match the surgical approach. An ALIF talk needs the great vessels and the L4-5 / L5-S1 vascular window, with mobilization of the iliac vein and the position of the median sacral artery. A posterior lumbar fusion talk needs the pars interarticularis, the facet joint capsule, and pedicle entry points (Magerl, Roy-Camille). A cervical talk separates the anterior approach (Smith-Robinson plane, carotid sheath, recurrent laryngeal nerve, esophagus) from the posterior. Anatomic precision matched to the approach is the floor, not a stretch goal.
Classification slides that earn their place. Meyerding I–V for spondylolisthesis, Wiltse etiologic types (dysplastic, isthmic, degenerative, traumatic, pathologic, post-surgical), Lenke 1–6 for AIS, SRS-Schwab for adult deformity, Frankel/ASIA for spinal cord injury, Eden-Spengler for thoracic disc herniation, Tomita and Tokuhashi for metastatic disease, AO Spine for thoracolumbar trauma. If a classification doesn't change management on the next slide, drop it. If it does, show it with case examples.
Imaging slides with the right modalities. Standing 36-inch scoliosis films, flexion-extension laterals for instability, dynamic MRI when stenosis is positional, CT for bony anatomy and fusion assessment, MRI for neural elements and Modic signal, DEXA for fixation planning in osteoporotic bone. A deformity talk that uses recumbent X-rays instead of standing films telegraphs lack of depth.
Technique comparisons with structured trade-offs. ALIF vs posterior fusion vs lateral (LLIF/XLIF) vs OLIF isn't an opinion question — each has objective trade-offs (lordosis correction, cage footprint, neural element risk, vascular access risk, indirect vs direct decompression, ability to reduce spondylolisthesis). A two-column or three-column comparison slide with consistent headers beats prose.
Outcomes data with confidence intervals, not point estimates. Fusion rates, ODI improvement, VAS reduction, SF-36, reoperation rates, infection rates — show the trial, the n, the timepoint, and the CI. A "70% fusion rate" floating in a bullet is a footnote in a journal article and a credibility leak in a presentation.
Complications slides that name the avoidance maneuver. "Dural tear" is a complication; "primary repair with 6-0 Prolene, fibrin glue, 24-hour bed rest, lumbar drain only if persistent leak" is the technique. Same for vascular injury during ALIF (vascular access surgeon on standby, CTA pre-op for redo cases), screw malposition (intra-op CT or fluoro-CT navigation, neuromonitoring with stim-EMG), pseudarthrosis (biologics selection, post-op brace, smoking cessation), and adjacent segment disease (sagittal balance restoration, semi-rigid fixation considerations).
Image-rich without being a stock-photo gallery. Imaging plates, intra-op photos, instrumentation renderings, technique diagrams. Skip the surgeon-in-blue-scrubs stock cliché — NASS, AAOS, and SRS audiences ignore it.
Step-by-Step: Building Your Spine Surgery Lecture with ChatSlide
1. Pick the right scenario
In ChatSlide, choose Conference > Workshop for NASS instructional courses, AAOS specialty days, SRS half-day instructional courses, or industry-sponsored teaching sessions. The outline biases toward the technique-primer → classification → comparison → outcomes → complications → pearls structure these audiences expect.
For a fellowship didactic, use Education > Lecture. The structure shifts toward primer-heavier, with classification, exam, and imaging slides earlier and more space for the trainee-level pearls.
For an academic conference talk on a single technique innovation, use Conference > Keynote. For an M&M case presentation, General > General with explicit prompting for the root-cause analysis section. For a tumor-board case (metastatic spine disease, primary bone tumor, intradural lesion), Conference > General with explicit multidisciplinary framing.
2. Write the topic the way you'd brief your fellow
Generic strings produce generic decks. Compare:
- Bad: "Spine fusion lecture"
- Better: "ALIF vs posterior fusion for spondylolisthesis"
- Best: "L4-5 / L5-S1 high-grade dysplastic spondylolisthesis: ALIF with posterior fixation vs Smith-Petersen / sacral dome osteotomy with posterior fusion — 45-min NASS instructional course with case examples and 2-year ODI / fusion-rate outcomes"
The third version gives the AI enough to build a 28-slide deck weighted correctly for a mixed orthopedic / neurosurgical spine audience — heavier on technique comparison and outcomes, lighter on basic anatomy primer.
3. Define the audience precisely
"Spine surgeons" is too generic. Be explicit:
- "PGY-4 orthopedic spine fellows on their adult deformity rotation"
- "Mixed orthopedic and neurosurgical spine fellows at a NASS instructional course"
- "Community spine surgeons attending AAOS specialty day on degenerative cervical myelopathy"
- "Spine tumor board attendees: spine surgery, radiation oncology, medical oncology, pathology"
- "Pain medicine fellows learning indications for BVNA in chronic vertebrogenic low back pain"
- "M&M conference: faculty and residents reviewing a postoperative spine infection root cause"
A fellow deck spends real time on classification systems and pearls; an M&M deck spends 90% on the case, the decision points, and the avoidance maneuver.
4. Generate the outline first
Outline generation is fast. Read the section structure before committing to slides. Common spine edits:
- Add an explicit "imaging interpretation" section if the deck is image-heavy (deformity, tumor, trauma)
- Combine redundant primer sections (one lumbar anatomy slide is enough for an experienced audience)
- Move outcomes data adjacent to the technique comparison, not three sections later
- For technique-focused decks, add a "step-by-step intra-op" section with explicit setup, exposure, decompression, instrumentation, closure subsections
- For NASS / AAOS instructional courses, add a "pearls and pitfalls" closing — the audience expects a 5-bullet summary they can photograph
5. Generate slides with images
This is the step where generic AI tools fall down hardest. They produce text slides with stock-photo surgeons in scrubs. ChatSlide's image step pulls in spinal anatomy diagrams, sagittal and axial imaging plates, instrumentation renderings, and technique diagrams — the visual vocabulary spine audiences expect.
For modality-specific imaging (your own intra-op photos, the patient's standing scoliosis films, post-op CT confirming hardware position, fusion-assessment CT at 1 year), swap in your own de-identified images. The deck structure stays intact — drop your DICOMs into the existing image slots. ChatSlide does not see your raw DICOMs or PHI; de-identify at the source.
6. Refine for the room
A 45-minute NASS instructional course slot reads differently than a 7-minute M&M case. Tighten the deck for the room:
- NASS / AAOS instructional course: 25–35 slides, technique-comparison heavy, two-three case examples, outcomes table with CIs
- Fellowship didactic: 22–28 slides, classification-heavy, exam and imaging slides earlier, pearls at the end
- SRS half-day instructional course: 30–40 slides, deformity-focused, standing 36-inch films throughout
- M&M case presentation: 10–14 slides, case timeline-driven, explicit root-cause / avoidance slide
- Tumor board case presentation: 8–12 slides, multidisciplinary framing, imaging-heavy, treatment-option matrix
- Industry-sponsored teaching session: 18–24 slides, technique-focused, indications-and-results balanced
- Patient counseling deck (pre-op): 6–10 slides, large text, surgical plan diagram, expected timeline, red flags
7. Export to PPTX or present from the browser
Exported PPTX preserves layout, bullets, and image positions — useful when the conference room AV requires a local file. The browser preview also works well in the surgeon's office when reviewing the operative plan with a patient, where swapping slides live based on the patient's question matters more than the AV polish.
Specific Use Cases This Replaces
ALIF vs posterior fusion comparison for spondylolisthesis. Side-by-side approach anatomy, lordosis-correction comparison, indirect vs direct decompression discussion, fusion-rate and ODI outcomes at 1 and 2 years, complications profile (vascular access vs neural element risk), pearls on patient selection (BMI, prior abdominal surgery, vascular anatomy).
Sacral dome osteotomy / Smith-Petersen osteotomy for high-grade dysplastic spondylolisthesis. Indication framing (Meyerding III–V dysplastic), pre-op planning (standing 36-inch films, sagittal vertical axis, pelvic incidence-lumbar lordosis mismatch), technique steps (laminectomy, sacral dome resection, reduction maneuver, fixation), neuromonitoring (SSEPs, MEPs, free-run EMG), 2-year fusion and reoperation outcomes.
Modic Type 1 changes and basivertebral nerve ablation (BVNA / Intracept). Vertebrogenic low back pain physiology, Modic classification on MRI (Type 1 edema, Type 2 fatty, Type 3 sclerotic), patient selection (Modic 1 or 2, ≥6 months chronic LBP, conservative care failed), procedure technique (transpedicular approach, RFA probe placement at the basivertebral nerve terminus), SMART and INTRACEPT trial outcomes at 2 and 5 years.
Cervical disc arthroplasty vs ACDF. Indications (1-2 level cervical radiculopathy or myelopathy), patient-selection criteria (motion preservation candidates, facet status, ossification), implant options, 7-10 year heterotopic ossification and adjacent-segment data, reoperation rate comparison.
Adult spinal deformity (ASD) surgical planning. SRS-Schwab classification, sagittal alignment goals (PI-LL within 10°, SVA <5cm, PT <20°), osteotomy decision tree (Smith-Petersen vs pedicle subtraction vs vertebral column resection), fusion-level selection, complication-rate framing.
Minimally invasive lateral interbody fusion (LLIF / XLIF / OLIF). Approach corridor anatomy (psoas, lumbar plexus, retroperitoneal vessels), patient selection (L1-2 through L4-5, contraindicated at L5-S1), neuromonitoring during psoas dissection, cage selection and footprint, indirect decompression evidence, complication profile (transient psoas weakness, anterior thigh dysesthesia, vascular).
Metastatic spinal cord compression (MESCC) tumor board case. SINS spinal instability score, Tomita and revised Tokuhashi scoring, separation surgery + SBRT framing, NOMS framework (neurologic, oncologic, mechanical, systemic), surgical decision (decompression, posterior stabilization, vertebrectomy), radiation oncology coordination.
Cervical myelopathy: laminoplasty vs laminectomy and fusion vs anterior approach. mJOA and Nurick scoring, imaging characteristics, surgical decision tree (sagittal alignment, number of levels, K-line, OPLL presence), outcomes by approach.
Spine M&M case presentation. Case timeline (pre-op evaluation → intra-op decision → post-op course → complication → diagnosis → management), explicit decision-point slide, root-cause framing, system-vs-individual avoidance maneuver, take-home for the program.
Postoperative spine infection management. Risk stratification, organism profile, surgical vs non-surgical decision, role of hardware retention vs removal, antibiotic suppression duration, the role of plastic surgery for soft-tissue coverage.
Direct Research Database Access
ChatSlide's Research tab connects to the databases spine surgeons use daily:
- PubMed: Search by keyword, PMID, or DOI. Find the landmark trials, recent publications, and clinical guidelines relevant to your case. The AI reads abstracts and incorporates key findings into your slides with citations.
- Google Scholar: When your topic spans disciplines — say, the intersection of biomechanics and clinical outcomes — Scholar captures the broader academic literature that PubMed alone might miss.
- Clinical Trials (NCT): Presenting on a treatment where pivotal trials are ongoing? Search by NCT number or condition to pull trial design, endpoints, and status into your slides.
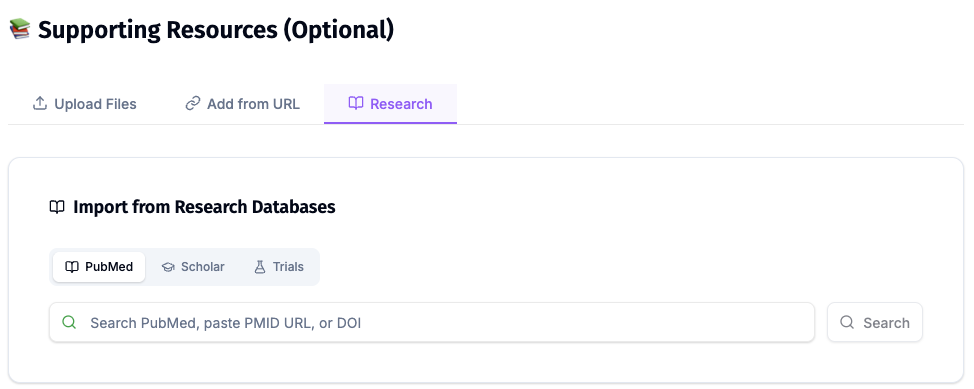
For spine specifically, the Research tab is most useful for pulling in the SPORT trial data on spondylolisthesis and stenosis, the SMART / INTRACEPT trials on BVNA for vertebrogenic LBP, the Lenke and SRS-Schwab classification primary citations, the Bridwell osteotomy descriptions, the IDSA spinal infection guidelines, and the AANS/CNS Guidelines for the Management of Acute Cervical Spine and Spinal Cord Injuries.
Tips Specific to Spine Lectures
Lead with the patient and the standing image, not the classification. Even an advanced audience responds to the patient image — a standing 36-inch deformity film, a flex-ex lateral showing slip progression, a sagittal MRI showing Modic Type 1 — far better than to a classification table dropped in cold.
Show the surgical plan as a diagram, not a paragraph. A two-panel "pre-op plan vs post-op result" diagram beats four bullets describing the same plan. NASS audiences respond to visual planning; M&M audiences need to see the actual decision being made.
Mark the outcome timepoints visibly. "Fusion rate" without a timepoint is meaningless. A horizontal timeline with 6-week, 6-month, 1-year, 2-year, and 5-year fusion and PROs marked beats four prose bullets and prevents the audience from chasing the data later.
Put complication avoidance on the same slide as the complication. "Vascular injury 0.5–1.5%" floating alone invites a hand-raise. "Vascular injury 0.5–1.5% — mitigated by access surgeon, pre-op CTA in redo cases, gentle iliac vein retraction medial to lateral" closes the loop on the same slide.
Cite NASS, AANS/CNS, and SRS guidelines where applicable. Society-endorsed pathways carry weight in cross-specialty conversations and with payers reviewing prior authorizations. Footer references to the NASS coverage policy on a procedure are worth two extra bullets of evidence prose.
Avoid the surgeon-in-blue-scrubs slide. Generic surgical stock photos signal you didn't put time into the talk. Imaging plates, intra-op photos, instrumentation renderings, and technique diagrams are the visual vocabulary spine audiences expect.
Build a 6-slide patient-counseling version of every major procedure. Once your fellowship didactic on adult deformity surgery is built, clone it into a patient-facing 6-slide deck — what the surgery is, why we recommend it, the expected timeline, the major risks, the recovery, the red flags. Hand the PDF out at the pre-op visit; patient understanding and consent quality improve measurably.
Why Generic AI Presentation Tools Underperform Here
Most AI deck generators were built for sales pitches and marketing decks. They optimize for visual flair and ignore the structural conventions of surgical didactics — and especially the conventions of spine. For a spine audience, generic tools produce:
- Anatomy slides that show "a spine" without labeling the pedicle entry points, the pars, or the great-vessel relationships
- Technique slides without a comparison column, so a fusion-options talk becomes a list of names rather than a decision aid
- Outcomes slides that report "70% improvement" with no n, no timepoint, no confidence interval — credibility-leaking on contact with an academic audience
- Complications slides that name the complication and stop there, with no avoidance maneuver or mitigation strategy
- Stock-photo "surgeon in OR" slides that have no place in a NASS instructional course or an M&M
- No classification depth at all, which guts the rationale behind every surgical decision
ChatSlide's clinical scenarios — Conference > Workshop, Conference > Keynote, Education > Lecture, General > General — bias the output toward the conventions spine audiences actually expect. You're still the surgical author; the tool just stops fighting your format.
Get Started
Building your next spine surgery lecture or case presentation on ChatSlide takes about as long as a clinic block. Drop a topic, refine the outline, generate the slides with spine imagery, swap in your own de-identified imaging and intra-op photos, and you have a NASS-, AAOS-, or fellowship-ready deck before the next OR day.
Try it free at chatslide.ai — most orthopedic and neurosurgical spine surgeons go from blank screen to first draft in under fifteen minutes.
Related guides:
- AI Medical Presentation Maker for Healthcare Professionals
- Medical Grand Rounds Presentation AI Guide
- Podiatry Presentation AI Guide
- Research Conference Presentation AI Guide
- Journal Club Presentation AI Guide
A note on patient data and HIPAA. ChatSlide's standard plans are not a HIPAA-covered service — keep PHI out of slide content, prompts, and uploads. De-identify your imaging, intra-op photos, and case data before you import. For hospital systems, academic spine programs, and multi-site orthopedic and neurosurgical practices that need a Business Associate Agreement, our Enterprise plan offers HIPAA-compliant deployment options — contact us to discuss BAA terms, SSO, and private-cloud or on-prem hosting.