Quick Answer: A strong obesity medicine lecture in 2026 covers (1) the disease model — adiposopathy, set-point, energy balance, and why "eat less, move more" failed for decades, (2) staging — BMI plus AACE Adiposity-Based Chronic Disease (ABCD), Edmonton Obesity Staging System (EOSS), waist-to-height, (3) lifestyle and behavioral foundation — MNT, motivational interviewing, sleep, stress, alcohol, (4) incretin-based pharmacotherapy — semaglutide (STEP, SELECT), tirzepatide (SURMOUNT-1/2/3/4), retatrutide, oral orforglipron, (5) legacy and second-line agents — phentermine/topiramate, naltrexone/bupropion, orlistat, setmelanotide, (6) metabolic-bariatric surgery — sleeve, RYGB, SADI/OAGB, indications under the 2022 ASMBS/IFSO guidelines, durability, and the surgery-vs-GLP-1 conversation, and (7) special populations — peri-conception, adolescents, post-bariatric weight regain, cardiometabolic risk reduction. Target 25–35 slides for grand rounds, 12–15 for a focused clinic-staff or ABOM review session. ChatSlide accepts the STEP/SURMOUNT/SELECT trial PDFs and the AACE/Obesity Society guidelines and produces the structured lecture format obesity medicine programs expect.
The Obesity Lecture Tax in 2026
Obesity medicine in 2026 is the fastest-moving subspecialty in adult internal medicine. The American Board of Obesity Medicine (ABOM) certifies thousands of physicians a year, GLP-1 receptor agonists have moved into cardiovascular and renal indications, and the SURMOUNT and SELECT data have rewritten how primary care, endocrinology, and bariatric surgery talk to each other. A weight-management clinic that gave the same noon conference two years ago is now obsolete by half.
That moves the deck-building problem from "once a year" to "every quarter." A single endocrinology grand rounds on tirzepatide pulls from four landmark trials, two FDA labels, the 2023 AHA scientific statement, the 2022 ASMBS/IFSO consensus, and the latest ADA Standards of Care. A bariatric surgery M&M needs operative video stills, comorbidity-resolution tables from ASMBS-MBSAQIP, and a clear comparison against pharmacotherapy. Multiply that by quarterly journal clubs, ABOM CME requirements, MOC modules, and patient-education sessions — and obesity medicine has quietly become one of the most slide-heavy clinical practices anywhere.
Build the deck the old way and you spend Saturday hunting for a clean weight-trajectory graph from STEP-1, redrawing the GLP-1/GIP receptor mechanism in PowerPoint, and copying NNT/NNH numbers from supplementary tables. By Sunday afternoon the deck is half-built and the senior physician already changed the dose-escalation question they want you to address.

ChatSlide collapses the assembly step. Drop a topic — "GLP-1 receptor agonists vs metabolic-bariatric surgery for class III obesity" or "ABOM board review: pharmacotherapy" — and you get a structured lecture deck with a clear arc, mechanism diagrams, trial-comparison tables, and speaker-ready talking points. You stay in charge of the clinical judgement and the patient cases; the tool stops eating your weekend.
What a Strong Obesity Medicine Lecture Actually Needs
Obesity medicine audiences are unusually mixed. A first-year endocrinology fellow, a primary care physician chasing ABOM credits, a bariatric surgeon, a registered dietitian, and a behavioral health clinician will all be in the same room — and they all hate the same things. A board-quality obesity medicine deck has to hit a specific set of bars:
Frame obesity as a chronic disease, not a willpower failure. The disease-model slide gets reused in every obesity lecture ever given. It still needs to be there because half of every audience — clinicians included — still carries an "eat less, move more" mental model. Adiposopathy, set-point theory, the homeostatic vs hedonic drive, and the genetic contribution (PCSK1, MC4R, leptin pathway) belong on the first three slides. Lead with the biology and the rest of the talk lands differently.
Staging beyond BMI. BMI is necessary, never sufficient. Modern lectures show ABCD staging from AACE, the Edmonton Obesity Staging System (EOSS), and waist-to-height ratio side-by-side with the BMI cut-points. A 28 kg/m² patient with NAFLD, OSA, hypertension, and prediabetes is a more urgent intervention than a 32 kg/m² metabolically healthy patient — and your staging slide should make that obvious without saying it.
Pharmacotherapy slides that respect the data hierarchy. Semaglutide 2.4 mg has STEP-1 through STEP-8 plus SELECT for MACE. Tirzepatide has SURMOUNT-1 through SURMOUNT-OSA, SURMOUNT-MMO ongoing. Retatrutide has TRIUMPH-1/2/3 in motion. Oral orforglipron has ATTAIN. A strong deck shows weight loss at week 68/72, the responder-rate Sankey diagrams, the cardiovascular outcomes where they exist (SELECT, FLOW, STEP-HFpEF), and explicit NNT/NNH numbers. Bullet-only pharmacotherapy slides get destroyed in Q&A.
Surgery vs medication, presented honestly. The single most-asked question in 2026 is "do my patients still need surgery if GLP-1s exist?" The honest answer requires a side-by-side: durability past 5 years, comorbidity remission (T2D, hypertension, OSA, NAFLD/MASH), cost-effectiveness, access barriers, and the post-medication regain data (STEP-1 extension, SURMOUNT-4 withdrawal). A deck that ducks this comparison loses the room.
Special populations. Adolescents (semaglutide ≥12 per STEP-TEENS, sleeve gastrectomy per AAP 2023), pre-conception and pregnancy (washout, switch-to-metformin), older adults (sarcopenic obesity, lean mass preservation, resistance training), and post-bariatric regain need their own slides. Generic "individualize therapy" lectures don't move clinical practice.
Step-by-Step: Building the Lecture with ChatSlide
The workflow is roughly the same whether you're building a 60-minute grand rounds or a 20-minute fellowship didactic.
1. Start with the topic and the audience. "Obesity medicine grand rounds: GLP-1 receptor agonists, triple-agonists, and metabolic-bariatric surgery in 2026" tells ChatSlide what you want. Naming the audience — endocrinology fellows + bariatric surgeons + primary care providers preparing for ABOM — calibrates the depth. A talk to medical students gets adiposopathy basics; a talk to bariatric surgeons gets the SADI vs RYGB durability head-to-head.
2. Choose the scenario. ChatSlide differentiates between Conference|Keynote (grand rounds, society meetings), Education|Lecture (course teaching, didactics), Education|Assessment (board review, MOC modules), Conference|ConfWorkshop (CME hands-on, motivational-interviewing workshops), and General|General (mixed-audience clinic talks). Pick the one that matches the room.
3. Bring your sources. Drag in the STEP-1, SURMOUNT-1, and SELECT PDFs, the latest AACE algorithm, the 2022 ASMBS/IFSO indications, and any of your own teaching files. ChatSlide reads them, extracts numerical results, and surfaces graphics and tables. You always get the option to review citations before they land in the deck.
4. Let the outline generate. A 6-section / 3-subpoint outline produces ~25–30 slides — a reasonable grand rounds length. For ABOM board prep, switch to 8–10 sections with 2 subpoints each; the deck gets shorter per topic but covers wider ground.
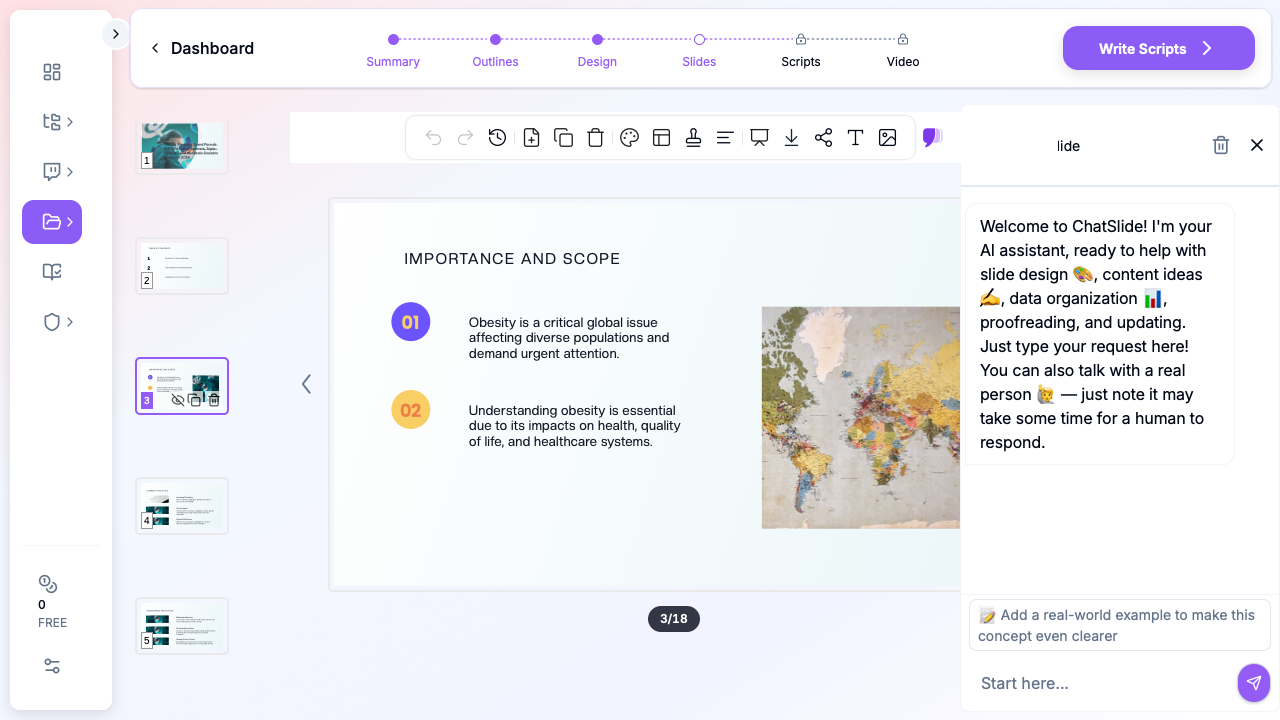
5. Edit at the slide level. The slide-chat feature accepts targeted edits: "add a side-by-side table of semaglutide 2.4 mg vs tirzepatide 15 mg weight loss at 68 weeks," "swap this stock image for the SURMOUNT-1 weight-trajectory graph I uploaded," "add a slide on retatrutide TRIUMPH-1 phase 2 data." Each edit happens in place — no rebuild, no re-imports.
6. Add speaker notes. ChatSlide auto-generates presenter notes that match the slide arc — not the bullet text. For obesity lectures the notes are especially useful because the bullet text is intentionally sparse and the real teaching happens off-slide ("this is where I'd anchor on the 21% weight loss number in SURMOUNT-1 and contrast against the 17% in STEP-8 oral").
Direct Research Database Access
ChatSlide's Research tab connects to the databases physicians use daily:
- PubMed: Search by keyword, PMID, or DOI. Find the landmark trials, recent publications, and clinical guidelines relevant to your case. The AI reads abstracts and incorporates key findings into your slides with citations.
- Google Scholar: When your topic spans disciplines — say, the intersection of genetics and oncology — Scholar captures the broader academic literature that PubMed alone might miss.
- Clinical Trials (NCT): Presenting on a treatment where pivotal trials are ongoing? Search by NCT number or condition to pull trial design, endpoints, and status into your slides.
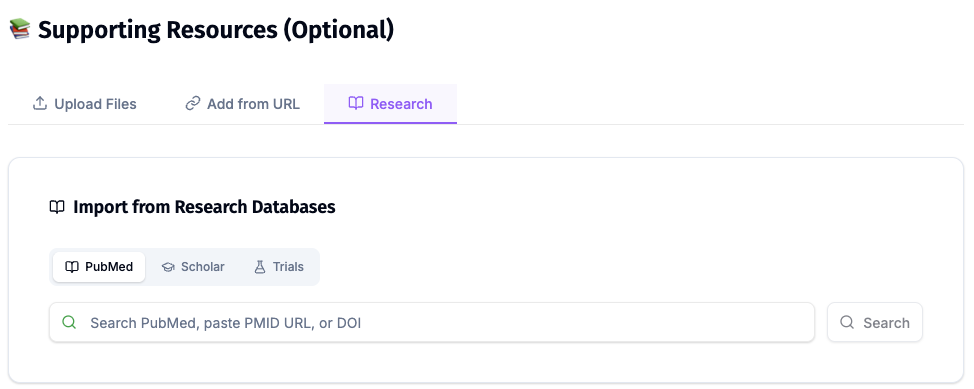
For obesity medicine specifically, the Research tab is most useful for pulling in STEP-1 (NCT03548935), SURMOUNT-1 (NCT04184622), SELECT (NCT03574597), SURMOUNT-MMO (NCT05556512), TRIUMPH-1 (NCT05882045), the FLOW renal-outcomes trial, the 2023 AHA Pathophysiology scientific statement, the 2022 ASMBS/IFSO consensus, the 2024 ADA Standards of Care Section 8, and the AACE 2023 Obesity Algorithm.
Tips Specific to Obesity Medicine Lectures
Always show responder curves, not just mean change. A "mean 15.3% weight loss" line undersells how good a GLP-1 is. The STEP-1 and SURMOUNT-1 responder-rate diagrams (% achieving ≥5%, ≥10%, ≥15%, ≥20% loss) are dramatically more persuasive — and more honest about the non-responder tail.
Make the AOM ↔ MBS handshake explicit. Most weight-management clinics now operate in a stepped-care model: lifestyle + AOM first, surgery for sub-optimal responders or patients with severe comorbidities. A single decision-tree slide showing when to escalate to surgery, when to bridge AOM to surgery, and when to add AOM after bariatric weight regain is the most-screenshotted slide in any obesity grand rounds.
Address access realistically. Insurance coverage, PA criteria, and the global supply situation are unavoidable in 2026. A slide on real-world access — Medicare carve-outs, employer coverage, prior-authorization friction, telehealth prescribing rules, compounded semaglutide warnings — keeps the lecture grounded in what your audience will actually see in clinic Monday morning.
Use case-based teaching for adolescents and pregnancy. STEP-TEENS opens with a 14-year-old with class II obesity, NAFLD, and prediabetes. SURMOUNT-MMO patients have established cardiovascular disease. Pre-conception cases anchor the washout and switch-to-metformin discussion. Two or three case slides beat any number of bullets.
Cite the de-prescribing data. STEP-1 extension and SURMOUNT-4 are now mandatory citations. The 2/3-regain pattern after withdrawal is the strongest argument for long-term therapy framing — and the most common Q&A target. Have the graphs on hand.
A note on patient data and HIPAA. ChatSlide's standard plans are not a HIPAA-covered service — keep PHI out of slide content, prompts, and uploads. De-identify case data and remove patient identifiers from any clinic-system screenshots before importing. For hospital systems, academic medical centers, and obesity medicine clinics that need a Business Associate Agreement, our Enterprise plan offers HIPAA-compliant deployment options — contact us to discuss BAA terms, SSO, and private-cloud or on-prem hosting.
Where This Lives in the Day-to-Day Practice
A weight-management physician we talked to summarized the workflow change: "I used to give one set-piece lecture a year. Now I give a quarterly update — STEP-8 in spring, SURMOUNT-4 in summer, retatrutide TRIUMPH in fall, the year-end ABOM MOC review in winter. Building four decks a year from scratch isn't sustainable."
The most common ChatSlide uses we see from obesity medicine practices:
- Quarterly grand rounds updates. New trial data drops, the deck gets rebuilt in 90 minutes instead of the weekend.
- ABOM board review series. A clinic with three ABOM candidates per cycle splits the curriculum into ~12 modules — pathophysiology, staging, behavioral, pharmacotherapy, surgery, special populations, MBS complications, post-op nutrition, anti-obesity medications during pregnancy, cardiometabolic comorbidities, pediatrics, regulatory/coding.
- Clinic-staff training. Dose-escalation protocols, sick-day rules, GLP-1 GI side-effect management, and post-bariatric vitamin/labs schedules turn into 8–12 slide deck for MAs and RNs.
- Patient-education sessions. Group visits on what to expect on a GLP-1, what to expect after sleeve gastrectomy, and how to navigate insurance. Same skeleton as the clinical deck, different voice.
- Multidisciplinary case conferences. Bariatric surgery, endocrinology, behavioral health, and primary care presenting the same complex patient. A shared deck with each specialty's view side-by-side cuts conference prep from a week to an afternoon.
Get Started
If you're building obesity medicine or weight-management presentations in 2026 — endocrinology grand rounds, ABOM board review, multidisciplinary clinic teaching, or patient-facing GLP-1 education — try ChatSlide for the next deck on your calendar.
Start your obesity medicine presentation →
If you teach across cardiometabolic territory or run a multidisciplinary clinic, our related guides are worth bookmarking:
- Patient education presentation AI — for GLP-1 and post-bariatric patient teaching
- Echocardiography presentation AI — for the cardiometabolic-imaging overlap
- Nephrology and critical care presentation AI — for the FLOW / SELECT renal/CV-outcomes audience