Quick Answer: A strong urology teaching deck usually moves through (1) the clinical problem and who it affects — epidemiology, presentation, and why the condition matters (BPH, prostate or bladder cancer, urolithiasis, bladder pain syndrome); (2) evaluation — focused history, exam, the right labs and imaging (PSA, urinalysis, uroflow/PVR, CT urogram, cystoscopy); (3) the decision framework — surveillance vs. medical vs. surgical management, and the trade-offs patients actually weigh; (4) the intervention — medical therapy, endoscopic options (TURP, HoLEP, ureteroscopy, PCNL), or extirpative/reconstructive surgery, with the anatomy and steps that matter; (5) evidence and guidelines — the AUA/EAU guideline and the trial behind each recommendation; and (6) outcomes, complications, and follow-up. Aim for 25–35 slides for grand rounds or an AUA instructional course, 18–22 for a resident didactic, and 8–12 slides for a patient-counseling or tumor-board case. ChatSlide takes your notes, a guideline PDF, or a landmark paper and drafts this structure with relevant imagery and cited claims.
The Challenge: Urology Spans Medicine and Surgery — and So Do the Slides
Urology is unusual: in a single clinic day you counsel a man on active surveillance for low-risk prostate cancer, manage a woman's overactive bladder medically, and book a ureteroscopy for an obstructing stone. The teaching load mirrors that breadth — a Tuesday resident didactic on voiding dysfunction, a GU tumor board where you present the surgical plan for a muscle-invasive bladder cancer, a patient-education evening on interstitial cystitis, an ABU board-review session on endourology.
Each of those needs a different deck, and the knowledge that makes you good in clinic and the OR is procedural, visual, and evidence-dense — exactly the kind that resists bullet points. You know the AUA risk-stratification for prostate cancer and the HoLEP enucleation sequence cold; turning either into 25 clean teaching slides is the part that eats an evening.
The usual options all fall short. Reusing last year's slide set teaches last year's guidelines — and urology guidelines move (PSA screening, MRI-targeted biopsy, GLP-1-era metabolic stone disease). Building from scratch means hunting for anatomy figures and formatting outcomes tables by hand. Generic AI slide tools produce confident text an attending will immediately flag as wrong — they'll conflate a radical with a simple prostatectomy, or invent a recurrence rate. ChatSlide is built for the opposite workflow: you bring the clinical substance, and it structures, illustrates, and sources the deck.
What Makes a Strong Urology Presentation
Whether the topic is BPH, prostate cancer decision-making, a bladder-pain-syndrome patient handout, or a stone-disease didactic, the best urology decks share a recognizable spine:
- Lead with the decision the patient or trainee faces. Urology is full of preference-sensitive choices: surveillance vs. treatment for low-risk prostate cancer, medical vs. surgical management of BPH, percutaneous vs. ureteroscopic stone removal. Frame the talk around those forks, not around a disease dump.
- Anatomy in the service of the management. Show the structures you actually act on — the prostatic urethra and bladder neck for a TURP, the neurovascular bundles for nerve-sparing prostatectomy, the ureteral course for stone work — rather than a textbook anatomy review.
- Evaluation that mirrors clinic. PSA kinetics, uroflowmetry and post-void residual, urinalysis and culture, CT urogram, cystoscopy, MRI/PIRADS — present the workup as the ordered sequence a clinician follows.
- Evidence for the controversial choices. When you claim MRI-targeted biopsy improves clinically significant cancer detection, or that a ureteral stent is unnecessary after uncomplicated ureteroscopy, name the trial. Urologists argue with data.
- Honest complications. Retrograde ejaculation after TURP, incontinence and erectile dysfunction after radical prostatectomy, stricture, sepsis after instrumentation — a teaching deck that omits them isn't teaching.
- A take-home algorithm. End with a one-slide decision tree the resident or patient can actually recall.
Step-by-Step: Creating Your Urology Presentation with ChatSlide
1. Start from what you already have. Upload a clinic note, a guideline PDF (AUA, EAU, NCCN), a chapter, or a landmark paper. If you only have a topic — "evaluation and management of microscopic hematuria" — start from that. ChatSlide reads the source rather than inventing content.
2. Set the audience and depth. A patient-counseling deck, a PGY-2 didactic, a fellows' instructional course, and a GU tumor-board case need very different depth. Tell the tool which one, and the outline calibrates — more anatomy and basics for juniors and patients, more nuance and evidence for fellows and attendings.
3. Review and edit the outline. ChatSlide generates a section outline first. This is where you, the urologist, do the high-value work: reorder the decision points, flag the controversy you want to teach, drop the section you'll handle live. Editing an outline takes minutes; editing 30 finished slides does not.
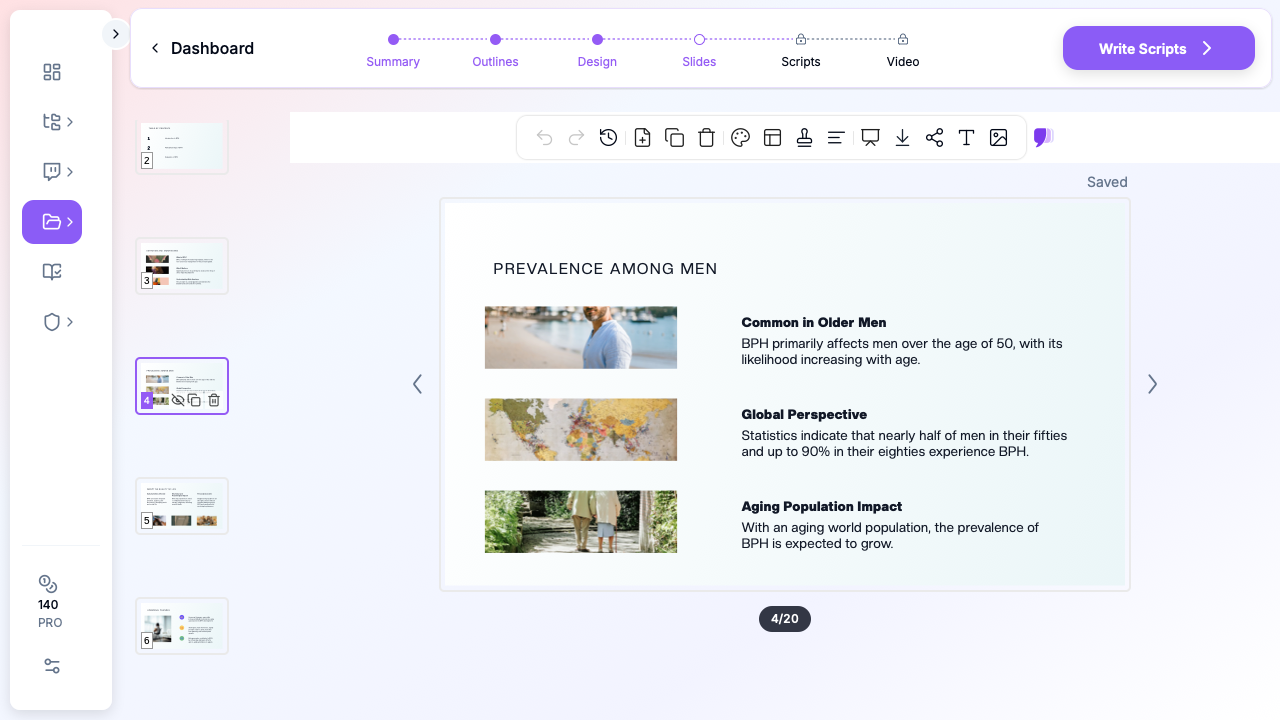
4. Generate slides with clinical imagery. The tool builds the deck with relevant images and lays out your evaluation sequences, technique steps, and comparison tables. Swap any image, adjust any layout.
5. Add charts for outcomes data. Stone-free rates by modality, PSA recurrence curves, IPSS improvement, complication rates — paste the numbers and ChatSlide builds clean charts instead of you wrestling with a spreadsheet.
6. Export for the venue. PDF for clinic handouts and distribution, PPTX or Keynote when you need to drop in a cystoscopy or surgical video clip or present from hospital hardware.
Direct Research Database Access
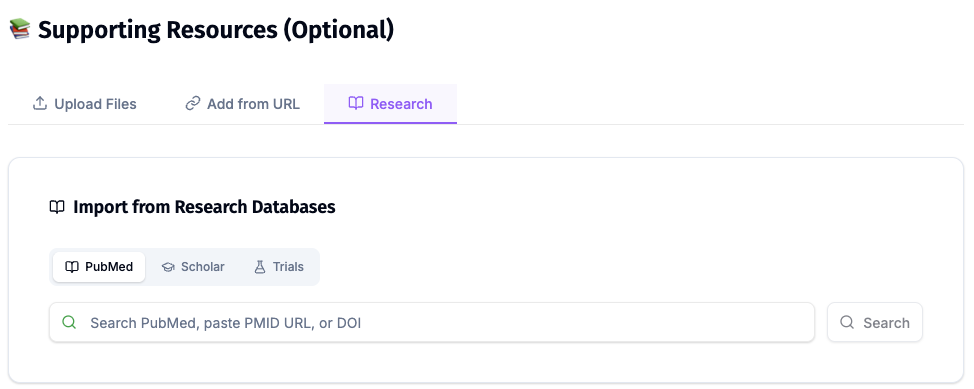
ChatSlide's Research tab connects to the databases physicians use daily:
- PubMed: Search by keyword, PMID, or DOI. Find the landmark trials, recent publications, and clinical guidelines relevant to your case. The AI reads abstracts and incorporates key findings into your slides with citations.
- Google Scholar: When your topic spans disciplines — say, the intersection of genetics and oncology — Scholar captures the broader academic literature that PubMed alone might miss.
- Clinical Trials (NCT): Presenting on a treatment where pivotal trials are ongoing? Search by NCT number or condition to pull trial design, endpoints, and status into your slides.
For a prostate cancer talk this is the difference between "MRI-targeted biopsy is better" and a slide that names the trial, the cohort, and the primary endpoint — the rigor an attending or board-review audience expects. For a stone-disease didactic it lets you pull the current AUA guideline and the supporting evidence in one pass.
Tips for Specific Urology Presentation Formats
Prostate cancer decision-making. This is fundamentally a shared-decision talk. Build the deck around risk stratification (PSA, Gleason/Grade Group, stage, genomics), then lay surveillance, surgery, and radiation side by side with their respective functional trade-offs. Patients and trainees both retain the comparison table.
BPH / LUTS. Move from symptom assessment (IPSS, uroflow, PVR) through medical therapy (alpha-blockers, 5-ARIs, combination) to procedural options (TURP, HoLEP, Rezūm, UroLift, aquablation), and keep the verb in the title for technique slides ("Enucleate the adenoma," "Resect to the capsule").
Bladder cancer, tumor board. You're one voice among medical oncology, radiation oncology, radiology, and pathology. Your slides should answer stage and grade, the proposed operation (TURBT, intravesical therapy, radical cystectomy with diversion), expected morbidity, and how neoadjuvant chemotherapy changes the plan — concisely.
Stone disease (urolithiasis). Pair the metabolic evaluation with the procedural decision (observation, MET, SWL, ureteroscopy, PCNL) and end with prevention. A clean stone-free-rate-by-size-and-location chart does a lot of teaching work.
Functional urology and patient education (OAB, incontinence, interstitial cystitis/bladder pain syndrome). Pitch to a patient or a junior trainee: plain-language mechanism, behavioral and medical first-line options, escalation (neuromodulation, intravesical therapy, Botox), and realistic expectations. Keep these short — 8 to 12 slides — and lead with what the patient can do this week.
ABU board review and resident didactics. Pitch to the exam and the clinic simultaneously. Pair each clinical point with the testable fact behind it, and keep guideline citations visible.
Note on patient data: ChatSlide's standard plans are not a HIPAA-covered service — keep PHI out of slide content and uploads. De-identify case material before you build a deck: no names, MRNs, dates of service, or identifiable images (including cystoscopy or pathology with embedded identifiers). For hospital systems, group practices, and clinics that need a Business Associate Agreement, our Enterprise plan offers HIPAA-compliant deployment options — contact us to discuss BAA terms, SSO, and on-prem / private-cloud hosting.
Get Started
The next didactic, tumor board, AUA course, or patient-education evening is already on your calendar. Instead of rebuilding slides between clinic and OR, bring your notes and the guideline, review the outline, and export a teaching-ready deck the same day.
Create your urology presentation with ChatSlide →
Keep PHI out of standard decks, lean on the Research tab so every claim traces to a source, and spend your prep time on the part only a urologist can do — the judgment between surveillance and the scalpel.